
Introduction
Rosacea perimenopause functional medicine — three words that rarely appear together in a conventional dermatology office, but that describe exactly what is driving the skin changes so many women in their 40s are experiencing and not getting answers for.
You’re in your 40s. Your skin has never been particularly sensitive — or maybe you’ve had mild rosacea for years that felt manageable. And then something shifts. The flushing becomes more frequent, more intense, harder to explain. Your skin reacts to things it never used to. Redness that used to come and go is now almost permanent. Triggers that never bothered you before suddenly set you off.
If this sounds familiar, perimenopause is almost certainly part of the picture — and it is almost never part of the conversation in a conventional dermatology office.
Perimenopause is not simply a hormonal transition. It is a systemic physiological shift that changes the internal environment of your body in ways that directly drive inflammatory skin conditions — rosacea in particular. In my functional medicine and functional dermatology practice, I see this pattern consistently: women in their late 30s and 40s who develop new or dramatically worsened rosacea, often alongside a constellation of other symptoms — weight gain, insomnia, brain fog, mood swings, hair loss, exhaustion — that they’ve been told are just part of getting older.
They are not just part of getting older. They are the expression of specific, identifiable, addressable imbalances. And the skin is often the most visible signal of all of them.
This post breaks down exactly what is happening hormonally and systemically during perimenopause that drives rosacea — including the critical distinction between early and late perimenopause, which produce different clinical pictures and require different approaches. Everything I cover here is informed by what I see in testing and in practice, and every protocol I build is individualized to what your specific results reveal.
Early vs. Late Perimenopause: Two Different Clinical Pictures
One of the most important and most overlooked distinctions in the perimenopause-rosacea conversation is that the hormonal pattern of early perimenopause is fundamentally different from that of late perimenopause and menopause — and those differences produce distinctly different rosacea presentations.
Early Perimenopause: The Erratic Estrogen Phase
In early perimenopause — typically the late 30s to mid-40s — estrogen does not simply decline. It fluctuates wildly. Cycles become irregular. Estrogen can surge to unusually high levels one month and drop sharply the next. This erratic pattern is hormonally chaotic, and the skin responds accordingly.
High estrogen states directly stimulate mast cells, triggering histamine release and vascular reactivity. When estrogen surges unpredictably, mast cells degranulate unpredictably — which is why women in early perimenopause often describe rosacea flares that seem completely random, impossible to connect to any consistent trigger. The trigger is internal and hormonal, not dietary or environmental.
Clinically, early perimenopausal rosacea tends to present as: unpredictable acute flares, intense flushing episodes that come and go, skin that seems reactive to everything without a clear pattern, and flares that correlate (often without the patient realizing it) with hormonal surges around ovulation or the luteal phase.
Additionally, many women experience relative estrogen dominance in early perimenopause — not necessarily because estrogen is absolutely high, but because progesterone begins to decline first, reducing its counterbalancing effect on estrogen’s stimulating activity. This relative dominance amplifies mast cell reactivity even further.
It is also worth noting that in some women, particularly those with gut dysbiosis, estrogen levels can be elevated through a different mechanism: disruption of the estrobolome — the subset of gut bacteria responsible for metabolizing and clearing estrogen. When gut dysbiosis impairs estrobolome function, deconjugated estrogen is reabsorbed into circulation rather than excreted, driving estrogen excess from the inside out. Bloating, irregular digestion, and gut discomfort are often the clinical tells for this pattern.
There is another layer that is almost never discussed in conventional medicine: xenoestrogens. These are endocrine-disrupting compounds found in plastics, pesticides, personal care products, and environmental chemicals that mimic estrogen in the body — binding to estrogen receptors and producing estrogenic effects even when a woman’s own estrogen levels are normal or even low. Because xenoestrogens are not detectable on a standard hormone panel, a woman can present with a full picture of estrogen dominance symptoms — rosacea flares, mast cell reactivity, histamine overload, mood changes — while her Hormone Zoomer shows estrogen within range. This is precisely why I run the Total Tox Burden panel alongside hormone testing. When we do, elevated endocrine-disrupting compounds frequently emerge as a significant part of the picture — and a driver that would have been completely invisible without it.
Late Perimenopause and Menopause: The Declining Hormone Phase
As perimenopause progresses into its later stages — and ultimately into menopause — the picture shifts. Estrogen is no longer surging erratically; it is declining, and declining significantly. Progesterone has fallen to very low levels. This produces a different inflammatory environment with a different rosacea presentation with more androgen dominance.
The acute, unpredictable flares of early perimenopause may give way to a more chronic, persistent baseline of skin reactivity and redness. The threshold for triggering a flare drops further — the skin becomes constitutionally more reactive — because the hormonal and immune architecture that once maintained equilibrium has fundamentally changed.
Progesterone, which functions as a natural mast cell stabilizer and anti-inflammatory agent, is now severely depleted. Estrogen’s decline removes its vascular protective effects while the mast cell-stimulating pattern established during the erratic estrogen phase continues. Insulin resistance — which increases as both estrogen and progesterone decline — creates ongoing endothelial damage and vascular instability. And the gut microbiome undergoes significant changes, further impairing histamine breakdown and estrogen clearance.
Clinically, late perimenopausal and menopausal rosacea tends to present as: more persistent, chronic redness rather than acute flushing episodes, increased skin sensitivity and dryness as the barrier weakens, and a broader symptom picture that includes hot flashes, sleep disruption, cognitive changes, and metabolic shifts — all expressing the same underlying hormonal collapse.
The Mechanisms: What Is Actually Driving the Inflammation
1. Progesterone Decline and Mast Cell Destabilization
Progesterone is one of the most underappreciated hormones in the rosacea conversation. Beyond its reproductive role, progesterone functions as a natural mast cell stabilizer — it actively suppresses mast cell degranulation and reduces histamine output. When progesterone declines during perimenopause, this stabilizing effect is progressively lost.
The result is a mast cell population that becomes increasingly reactive, degranulating more readily in response to stimuli that previously would not have triggered a response. This is a direct physiological explanation for why women who managed rosacea relatively well before perimenopause find it dramatically worsening during the transition — the hormonal brake on their mast cells has been released.
Bioidentical progesterone support — specifically a transdermal bioidentical progesterone cream applied topically — can be a meaningful part of addressing this imbalance. Unlike synthetic progestins, bioidentical progesterone closely mirrors the molecular structure of the body’s own progesterone and has a more favorable effect on mast cell regulation. I use Bio-Pro bioidentical progesterone cream in my functional medicine practice as part of an individualized protocol when the clinical and testing picture supports it. As always, any hormonal intervention is tailored to the individual and based on comprehensive testing.
2. Estrogen Dominance and Histamine Amplification
As discussed in the context of early perimenopause, high or erratically fluctuating estrogen directly stimulates mast cells and increases histamine production. But estrogen dominance during perimenopause is not always about absolute estrogen levels — it is frequently about the ratio of estrogen to progesterone, and about how well the body is clearing and metabolizing the estrogen it produces.
Poor estrogen clearance through Phase I and Phase II liver detoxification pathways allows estrogen metabolites to recirculate, amplifying the estrogenic load and its stimulating effect on mast cells. Gut dysbiosis compounds this by impairing the estrobolome, allowing deconjugated estrogen to be reabsorbed rather than excreted. Both patterns show up clearly on comprehensive hormone testing — which is why the Hormone Zoomer is central to my perimenopausal rosacea workup.
Supporting estrogen clearance and metabolism is a core component of the functional medicine approach to perimenopausal rosacea. This is where my functional medicine detox program plays an important role — anchored by NutriCleanse GHI, a medical food specifically formulated to support Phase I and Phase II liver detoxification and gut integrity, and SulforaOpti, which provides sulforaphane to upregulate the Nrf2 pathway and support both toxin and sex hormone metabolism. As with all interventions, the specific protocol is individualized based on testing and clinical presentation.

3. Cortisol, the HPA Axis, and the Stress-Inflammation Loop
The HPA axis — the hormonal communication system between the hypothalamus, pituitary, and adrenal glands — is significantly dysregulated during perimenopause. As ovarian hormone production becomes unpredictable, the adrenal glands are called upon to compensate, often increasing cortisol output in an attempt to maintain hormonal equilibrium.
Elevated cortisol has multiple consequences for rosacea. Cortisol directly activates mast cells and amplifies their degranulation response. It raises blood sugar — driving the endothelial damage and angiogenesis that sustain vascular rosacea. It suppresses the immune regulation needed to keep inflammatory signaling in check. And it creates a forward-feeding cycle: stress elevates cortisol, cortisol drives inflammation, inflammation worsens skin reactivity, visible skin worsening creates psychological distress, distress elevates cortisol further.
For perimenopausal women who are simultaneously managing work, family, sleep disruption, and the emotional weight of a body that feels unfamiliar, the HPA burden is significant. This is why stress physiology is not a soft add-on to the rosacea conversation — it is a hard clinical driver that warrants assessment and support.
4. Insulin Resistance and Endothelial Damage
Both estrogen and progesterone play roles in maintaining insulin sensitivity. As both hormones decline during perimenopause, insulin resistance increases — cells become less responsive to insulin, blood sugar rises, and the inflammatory consequences cascade through the body.
For the skin, chronic elevation in blood sugar damages the endothelial lining of blood vessels through glycation, promotes angiogenesis (the formation of new, fragile capillaries visible in rosacea), and sustains systemic inflammation. The characteristic vascular pattern of rosacea — persistent redness, visible capillaries, flushing — is in part an expression of this endothelial vulnerability.
This is why I consistently include a metabolic panel and lipid panel in my perimenopausal rosacea workup. Elevated cholesterol and LDL — which I see frequently in this patient population — are not unrelated to the skin picture. They are part of the same metabolic dysregulation driving endothelial damage and vascular instability. Addressing insulin sensitivity and metabolic health is directly relevant to rosacea resolution, not a separate clinical concern.
5. Gut Dysbiosis and the Estrobolome
The gut microbiome undergoes significant changes during perimenopause — reduced diversity, shifts in key bacterial populations, increased intestinal permeability. These changes have direct consequences for rosacea through multiple pathways.
Reduced DAO enzyme production in a compromised intestinal lining impairs histamine breakdown, allowing histamine to accumulate systemically. A disrupted estrobolome worsens estrogen dominance by allowing deconjugated estrogen to re-enter circulation. Increased gut permeability or leaky gut allows bacterial fragments (LPS) into the bloodstream, triggering systemic immune activation and amplifying mast cell reactivity. And reduced microbial diversity impairs the immune regulation needed to keep inflammatory signaling calibrated.
Bloating, irregular digestion, and gut discomfort — symptoms that many perimenopausal women experience and assume are unrelated to their skin — are often the clinical signal that gut-driven estrogen dysregulation is part of their rosacea picture.
6. Xenoestrogens and Toxic Burden
Environmental toxins — particularly xenoestrogens found in plastics, pesticides, personal care products, and household chemicals, heavy metals and mycotoxins — are endocrine-disrupting compounds that mimic estrogen in the body, binding to estrogen receptors and amplifying the estrogenic load without appearing on a standard hormone panel. A perimenopausal woman can present with a full clinical picture of estrogen dominance — mast cell reactivity, histamine overload, rosacea flares, mood instability, sleep issues — while her hormone testing shows estrogen within normal range. The missing variable is xenoestrogenic burden, which only surfaces on a Total Tox Burden assessment.
Beyond their estrogenic mimicry, environmental toxins are direct mast cell activators and impair Phase I and Phase II liver detoxification, reducing the body’s capacity to clear both endogenous estrogen and histamine. In perimenopausal women — whose detoxification capacity is already under increased demand from the hormonal transition — toxic burden can be the tipping point that shifts a subclinical inflammatory pattern into overt, treatment-resistant rosacea. It is also one of the most commonly missed drivers, precisely because it requires testing that falls outside the standard medical workup.
Beyond the Skin: Rosacea as Part of a Larger Pattern
One of the most important things I want perimenopausal women with worsening rosacea to understand is that their skin is rarely the only thing expressing these imbalances. The same hormonal, metabolic, and inflammatory drivers that produce rosacea are simultaneously producing symptoms throughout the body.
The pattern I see most consistently in perimenopausal rosacea patients includes:
- Weight gain around the waist and abdomen that doesn’t respond to diet or exercise — driven by insulin resistance and cortisol-induced fat storage
- Inability to lose weight or gain muscle mass — compounded by declining testosterone, which is critical for body composition
- Insomnia and disrupted sleep — driven by progesterone decline (progesterone has a direct calming, sleep-supporting effect), cortisol dysregulation, and blood sugar instability
- Hair loss — which can reflect both androgenic activity (the 5-alpha reductase pathway converting available androgens into DHT at the follicle level) and thyroid dysfunction, nutrient insufficiency, and inflammation
- Brain fog and memory difficulties — driven by insulin resistance, inflammation, disrupted sleep, and declining estrogen’s effect on neurotransmitter regulation
- Irritability, mood swings, and anxiety — reflecting progesterone decline, cortisol dysregulation, and disrupted serotonin and GABA signaling
- Exhaustion and low motivation — reflecting adrenal burden, mitochondrial stress, thyroid changes, and declining testosterone
When a woman comes to me presenting with rosacea and several of these symptoms, I am not looking at a list of separate problems. I am looking at a single systemic picture with multiple expressions — and the rosacea is often the most visible one. Addressing the internal drivers resolves the full picture, not just the skin.
A Patient Story: When the Skin Is Telling the Whole Story
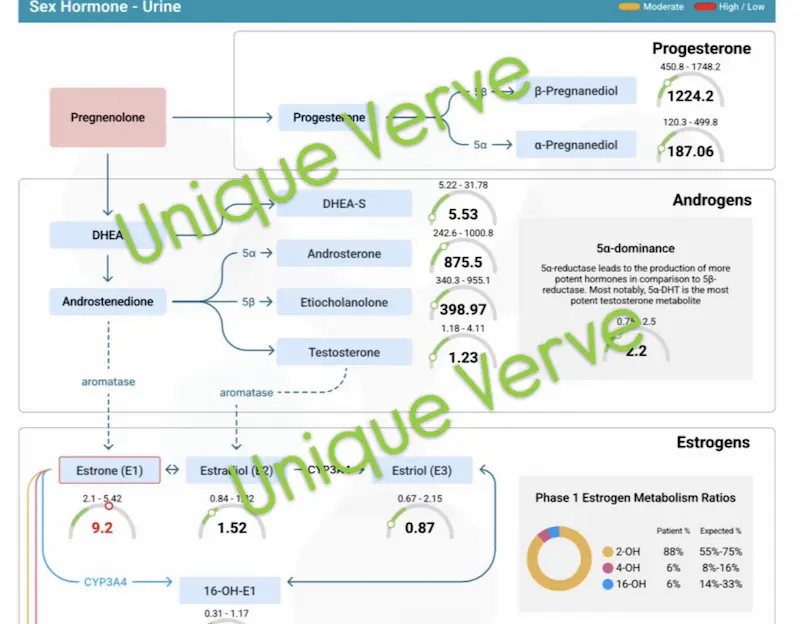
One of my patients came to me in her mid-40s with worsening rosacea — flushing, persistent redness, and increasing skin reactivity that had accelerated significantly over the previous two years. She had attributed the change to stress and aging. What she hadn’t connected to her skin: progressive weight gain around her waist despite no change in diet, complete inability to build muscle no matter how consistently she exercised, chronic insomnia, significant hair loss, brain fog that was affecting her work, and a level of irritability and exhaustion that felt foreign to her.
Comprehensive testing told a coherent story. Her Hormone Zoomer revealed high estrone (E1) — a pattern consistent with early perimenopausal estrogen elevation — driven in her case primarily by gut dysbiosis impairing estrobolome function. Her bloating, which she had mentioned almost as an afterthought, was the clinical tell. Elevated 5-alpha androsterone despite low free testosterone explained the paradox of her hair loss alongside weakness and low energy: her available testosterone was being preferentially converted through the 5-alpha reductase pathway, producing androgenic activity at the follicle (hair loss) without the systemic benefits of bioavailable testosterone (muscle, energy, motivation). Her lipid panel showed elevated total cholesterol and LDL — part of the same metabolic picture driven by increasing insulin resistance.
Her protocol addressed all of it systemically: gut restoration to rebalance the estrobolome and reduce the estrogenic load, estrogen clearance support through the functional medicine detox program including NutriCleanse GHI and SulforaOpti, bioidentical progesterone support with Bio-Pro to restore mast cell stabilization and improve sleep, and metabolic support to address insulin resistance and endothelial health. Topically, the emphasis was on barrier restoration and vitamin A reintroduction with Environ skincare.
Her rosacea improved significantly as her internal picture shifted. So did her sleep, her energy, her body composition, and her mood. None of these outcomes were separate — they were all downstream of the same upstream imbalances being addressed.
Rosacea Perimenopause Functional Medicine Approach: Internal and Topical
The internal protocol for perimenopausal rosacea targets the full hormonal, metabolic, and inflammatory picture — not just the skin. The topical approach prioritizes barrier restoration and structural skin integrity. Both are always individualized to what testing reveals.
You Deserve More Than “It’s Just Hormones”
If your skin has changed in your 40s — and especially if that change has come alongside other symptoms you’ve been told to accept as part of aging — something specific is driving it. The functional medicine approach to perimenopausal rosacea is not about managing what you see on the surface. It is about identifying the hormonal, metabolic, gut health, and inflammatory pattern that is producing it — and addressing that pattern systematically.
This is the foundation of my functional dermatology practice. The skin is the signal. The work is internal.
The functional medicine approach to perimenopausal rosacea does not rely on antibiotics or prescriptions. It relies on understanding what your body is specifically doing — and building a protocol around that.
I offer virtual Initial Functional Medicine Health and Skin Assessments for women who are ready to look upstream. This is where we take a full picture of your health history, your current symptoms, and the patterns that connect them — and build a testing and treatment strategy specific to your body.
I am not acting in the capacity of a physician, licensed dietitian-nutritionist, or prescriber, and I do not diagnose or treat medical conditions. All functional medicine services are educational in nature and offered virtually. If you have concerns about your health, please consult your healthcare provider.
→ Book your Initial Functional Medicine Health and Skin Assessment
Frequently Asked Questions
Why does rosacea get worse during perimenopause?
Perimenopause creates a systemic shift toward a pro-inflammatory, insulin-resistant state that directly amplifies every internal driver of rosacea. Declining progesterone removes its mast cell-stabilizing effect, increasing histamine output and vascular reactivity. Erratically fluctuating estrogen in early perimenopause triggers unpredictable mast cell degranulation. Increasing insulin resistance drives endothelial damage and angiogenesis. Gut permeability increases, impairing histamine breakdown and estrogen clearance. And the body’s overall inflammatory threshold drops, making the skin constitutionally more reactive. These changes happen simultaneously and compound each other — which is why rosacea can worsen rapidly during this transition.
Is perimenopausal rosacea different from regular rosacea?
The underlying mechanisms are the same — mast cell activation, histamine overload, gut dysbiosis, estrogen dominance — but perimenopause creates a specific hormonal environment that amplifies all of them simultaneously. The clinical presentation also differs depending on the phase of perimenopause. Early perimenopause tends to produce unpredictable, acute flaring driven by erratically fluctuating estrogen. Late perimenopause and menopause tend to produce more chronic, persistent skin reactivity as estrogen and progesterone both decline. Identifying which phase a patient is in significantly shapes the approach.
Can progesterone help rosacea?
Yes — progesterone functions as a natural mast cell stabilizer and anti-inflammatory hormone. As progesterone declines during perimenopause, mast cells become increasingly reactive, producing more histamine and driving more vascular inflammation in the skin. Restoring progesterone support — using bioidentical progesterone rather than synthetic progestins, which have different receptor activity — can meaningfully reduce mast cell reactivity and improve rosacea alongside other perimenopausal symptoms. As with all hormonal interventions, this is individualized based on comprehensive hormone testing.
Why do I have rosacea and weight gain and hair loss at the same time?
Because they are all expressions of the same underlying hormonal and metabolic imbalances. Rosacea reflects mast cell activation and systemic inflammation. Abdominal weight gain reflects insulin resistance and cortisol dysregulation. Hair loss in perimenopausal women often reflects androgenic pathway activity — specifically testosterone being converted through the 5-alpha reductase pathway — alongside thyroid changes and nutrient insufficiency. All of these patterns emerge from the same perimenopausal hormonal shift. Addressing the root causes systemically tends to improve all of them, not just the skin.
What blood tests should I get for perimenopausal rosacea?
A comprehensive functional medicine workup for perimenopausal rosacea typically includes a full hormone panel assessing estrogen fractions, progesterone, testosterone, cortisol, and estrogen metabolism pathways; a metabolic panel and lipid panel to assess insulin resistance and cardiovascular risk; a gut microbiome assessment including estrobolome health and leaky gut markers; a full thyroid panel; and micronutrient testing with genetic SNPs. Standard dermatology testing does not include most of these panels — which is why the internal drivers of perimenopausal rosacea are so frequently missed.
How long does it take for perimenopausal rosacea to improve with functional medicine?
Meaningful improvement typically begins within 6–12 weeks of implementing a targeted protocol, with more significant and sustained improvement over 3–6 months as the underlying hormonal, gut, and metabolic imbalances are progressively addressed. The timeline varies depending on the complexity of the individual’s picture, the severity and duration of the imbalances, and how consistently the protocol is implemented. Because we are addressing root causes rather than suppressing symptoms, the results tend to be more durable — the improvement continues rather than reverting when treatment stops.
Written by Natalie Maibenko – a Certified Functional Medicine Practitioner and Master Esthetician with 22+ years of experience and founder of Unique Verve

As a Certified Functional Medicine Practitioner my Expertise Encompasses:
- Immune System: frequent illness, UTIs, yeast infections
- Allergies, Asthma
- Skin Problems: acne, cystic acne, rosacea, eczema, dermatitis, ichthyosis, psoriasis, vitiligo, melasma
- Inflammation: arthritis, rhinitis, joint & muscle pain, migraines, headaches
- Sleep Disturbunces, Insomnia
- Gut Problems: IBS/IBD, bloating, acid reflux, gas, constipation, diarrhea, parasites, fungal/yeast overgrowths
- Hormonal Imbalances: PCOS, PMS symptoms, weight problems/inability to lose weight, thyroid problems
- Hair Loss, Alopecia
- Mood Imbalances: anxiety, depression, irritability
- Metabolic Dysfunction, Insulin Resistance, Type 2 Diabetes
- Optimizing Wellness for Successful Pregnancy
- Autoimmune Conditions: Hashimoto’s thyroiditis, grave’s disease, reumatoid arthritis (RA), lupus, etc
- Bone Health: osteopenia/ osteoporosis
- Effective Anti-Aging Strategies without Injectables with the inside-out & outside-in approach
- Detoxification of Heavy Metals, Mycotoxins, Environmental Toxins
- Reversing Breast Implant Illness
- Preparation for the Explant Surgery and Optimization of Wellness & Vitality Post-Explant
With love and gratitude,
Natalie Maibenko
Functional Medicine & Skincare Expert – Helping You Take Control of Your Health and Achieve Lasting Skin Results Nationwide — Virtual Practice
Disclaimer: Information and content on this website is provided for educational purposes only, and is not intended to diagnose, treat and to be a substitute for the advice provided by your physician or other healthcare professional. No information offered here should be interpreted as a diagnosis of any disease, nor an attempt to treat or prevent or cure any disease or condition. If you have any concerns or questions about your health, you should always consult with a physician or other healthcare professional. Do not disregard, avoid, or delay obtaining medical or health-related advice from your healthcare professional. Always speak with your healthcare professional before taking any medications, supplements or pursuing any wellness programs. Information provided on this website does not create a doctor-patient relationship between you and any professional affiliated with this website.