Rosacea Root Cause Functional Medicine Approach: Stop Managing Symptoms, Address the Source, Clear Your Rosacea, Reclaim Your Health.

Introduction
If you’ve been managing rosacea for years — rotating through topical antibiotics, avoiding your favorite foods, and still watching your skin flare — you already know that conventional treatment isn’t getting to the bottom of it. Metronidazole and doxycycline can quiet the inflammation temporarily. But they don’t ask the question that matters most: why is your skin inflamed in the first place?
Rosacea is not a skin problem that happens to have some internal triggers. It is a systemic inflammatory condition that shows up on the skin. Until the upstream drivers are identified and addressed, the flares keep coming — often getting worse over time, especially as women move through perimenopause.
In my functional dermatology practice, I work with women who are frustrated with exactly this pattern. Their dermatologist has ruled out other conditions, their skincare routine is “perfect,” and yet their skin continues to flare. What we find, consistently, is a cluster of interconnected internal drivers that conventional medicine rarely investigates: mast cell activation, histamine overload, estrogen dominance, food sensitivities, blood sugar dysregulation, gut dysbiosis, and toxic burden. Often, all of them are present at once — because they feed each other.
This post walks through what those drivers are, why they’re so frequently missed, and what a true root-cause approach to rosacea actually looks like.
Why Conventional Rosacea Treatment Falls Short
The standard approach to rosacea centers on trigger avoidance, topical antibiotics like metronidazole, oral antibiotics like doxycycline, and — in more advanced cases — laser therapy. These tools can reduce visible redness and papules in the short term. But there are several fundamental problems with stopping here.
It treats the symptom, not the signal
Redness, flushing, and vascular reactivity are downstream expressions of internal inflammation. Suppressing them at the skin level doesn’t resolve the internal inflammatory cascade driving them. Think of it like turning off a fire alarm without addressing the fire.
Antibiotics disrupt the very system that protects you
Long-term use of oral antibiotics — a mainstay of rosacea management — decimates the gut microbiome. The gut is central to immune regulation, histamine breakdown, estrogen metabolism, and barrier integrity and to control systemic inflammation. Chronic antibiotic use can worsen dysbiosis, impair DAO enzyme production (which degrades histamine), and paradoxically amplify the inflammatory drivers of rosacea over time.
Trigger avoidance doesn’t explain why triggers became triggers
Wine, spicy food, sun, heat, chocolate — these are real rosacea aggravators for many women. But the more important question is: why has your reactivity threshold dropped so low that ordinary stimuli produce such an outsized response? The answer lies inside the body, not in the avoidance list.
Perimenopause is almost never part of the conversation
For women in their late 30s, 40s, and 50s who notice rosacea appearing or worsening, the hormonal transition is rarely explored. Yet the shift toward a pro-inflammatory, insulin-resistant state that characterizes perimenopause creates precisely the internal environment in which rosacea thrives. We’ll come back to this in detail.
What Actually Causes Rosacea: Why the Conventional Answer Is Incomplete
Conventional medicine identifies rosacea triggers — heat, alcohol, spicy food, UV exposure — but rarely asks what made the body so reactive to them in the first place. The answer lies in a cluster of internal drivers: mast cell activation, histamine overload, hormonal imbalance, gut dysfunction, food sensitivities, and toxic burden. These are the root causes. The next section walks through each one in detail.
The Root Causes of Rosacea: What’s Really Driving Your Flares
In functional medicine, we look at the body as an interconnected system. In rosacea, the upstream drivers tend to cluster and reinforce one another. Here is how they connect.
1. Mast Cell Activation and Histamine Overload
Mast cells are immune cells distributed throughout the body — including in skin tissue — that release histamine and other inflammatory mediators in response to perceived threats. When mast cells are chronically activated, the result is persistent vascular reactivity, redness, flushing, and facial inflammation. This is the central mechanism in rosacea.
The critical question is what is activating the mast cells. The most common upstream drivers I identify clinically include estrogen dominance, food sensitivities, toxic burden and gut dysbiosis — all of which we explore below. Treat the mast cell activation without addressing its drivers and you are managing the symptom, not the cause.
Histamine overload compounds the problem. When histamine is produced faster than the body can break it down — due to impaired DAO enzyme activity in the gut, poor liver clearance, or chronic mast cell degranulation — it accumulates systemically, amplifying the inflammatory response on the skin.
2. Estrogen Dominance
Estrogen directly stimulates mast cells and increases histamine output. High estrogen states — whether from excess production, poor clearance through the liver, or declining progesterone creating a relative dominance — are one of the most clinically significant and consistently overlooked drivers of rosacea I see in practice.
Estrogen dominance doesn’t require high absolute estrogen levels. It can occur when progesterone is low (progesterone normally counterbalances estrogen’s stimulating effects on mast cells), when liver detoxification is impaired and estrogen metabolites recirculate, or when the gut microbiome — specifically the estrobolome — is disrupted and reactivates estrogen that should have been cleared.
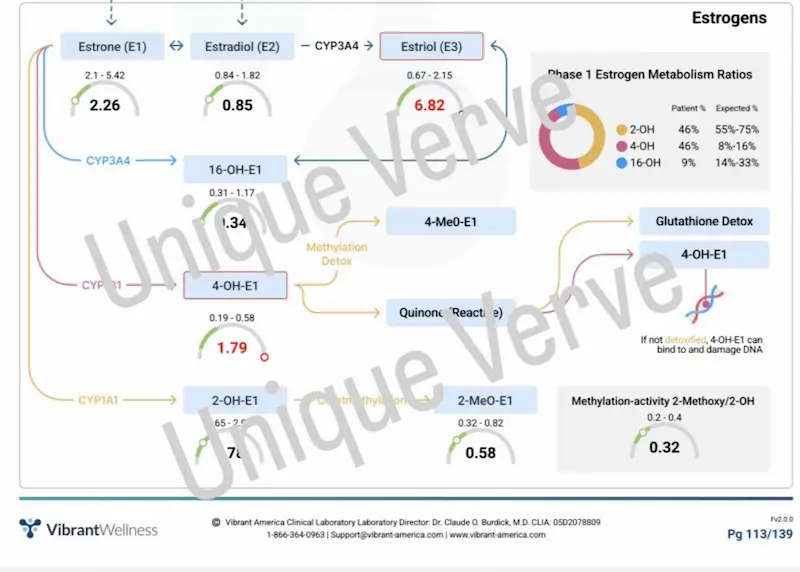
This is why I run the Vibrant Wellness Hormone Zoomer in virtually every rosacea case. We’re not just looking at estrogen and progesterone in isolation — we’re looking at the full picture of estrogen metabolism, clearance, and relative hormonal balance. The pattern I see most consistently: estrogen dominance in the context of lower progesterone and/or poor estrogen clearance.
3. Food Sensitivities: The Most Overlooked Driver
Food sensitivities are distinct from food allergies. They don’t produce an immediate IgE-mediated reaction. Instead, they create a low-grade, chronic immune activation — a steady release of stress hormones and inflammatory mediators that keeps the body in a state of reactivity.
Clinically, this matters for rosacea in several ways. Chronic immune activation from unidentified food sensitivities elevates stress hormones, which elevate blood sugar, which damages the endothelial lining of blood vessels and stimulates angiogenesis — the formation of new, fragile capillaries visible in rosacea. Unknown food sensitivities also contribute to gut permeability, dysbiosis, and mood imbalances — all of which compound the internal inflammatory load.
What makes this particularly important is that patients almost never connect a food they eat regularly to a skin symptom that shows up 24–72 hours later. Comprehensive food sensitivity testing often reveals patterns that have been silently driving inflammation for years.
4. Blood Sugar Dysregulation
Elevated blood sugar and insulin resistance are central to the inflammatory cascade underlying rosacea, and they are downstream of multiple drivers: estrogen dominance, food sensitivities, toxic burden, stress, and gut dysbiosis (the list might be different or may include other upstream triggers and/or root-causes in your unique case) all contribute to blood sugar instability.
When blood sugar is chronically elevated, it damages the endothelial lining of blood vessels through a process called glycation, promotes angiogenesis (formation of new blood vessels from pre-existing ones), and sustains systemic inflammation. For women in perimenopause — a period already characterized by increasing insulin resistance — this dynamic is especially relevant. The drop in estrogen and progesterone that occurs during this transition directly worsens insulin sensitivity, creating a compounding effect on rosacea severity.
Research adds an important dimension here: endothelial dysfunction is recognized as the first step in atherosclerotic disease, and emerging evidence confirms it is measurably present in rosacea patients. A published study found that flow-mediated dilation — a key marker of endothelial function — was significantly lower in rosacea patients compared to healthy controls, suggesting that rosacea is not a disease limited to the skin but one that may affect the cardiovascular system.
This is consistent with findings from systematic reviews linking rosacea to coronary artery disease, metabolic syndrome, and hypertension, as well as co-occurrence with inflammatory bowel disease, multiple sclerosis, Parkinson’s disease, and migraine. For this reason, patients presenting with rosacea warrant evaluation not just of skin drivers, but of early cardiovascular and systemic inflammatory risk.
5. Gut Dysbiosis and Leaky Gut
The gut-skin axis is well-established in the research: a disrupted gut microbiome consistently correlates with inflammatory skin conditions including rosacea. The mechanisms are multiple.
Leaky gut allows lipopolysaccharides (LPS) — fragments of gram-negative bacterial cell walls — to enter the bloodstream and trigger systemic immune activation. Dysbiosis impairs DAO enzyme production in the intestinal lining, reducing the body’s capacity to break down histamine. A disrupted estrobolome (the subset of gut bacteria that metabolize estrogen) allows deconjugated estrogen to be reabsorbed, contributing to estrogen dominance. Reduced microbial diversity alters immune regulation and amplifies inflammatory signaling.
This is why comprehensive gut assessment can be often quite valuable in my rosacea patient workup. The Gut Zoomer provides a comprehensive picture of microbiome composition, pathogenic load, inflammatory markers, and digestive function — data that is simply not available through conventional testing.
6. Toxic Burden
Environmental toxins — heavy metals, mycotoxins, pesticides, and other endocrine-disrupting compounds — are mast cell activators. They also impair liver detoxification, which is critical for both estrogen clearance and histamine metabolism. In women with significant toxic burden, addressing toxins is often a prerequisite for meaningful progress on the hormonal and inflammatory drivers of rosacea.
I assess total toxic burden through the Vibrant Wellness Total Tox Burden panel, which screens for heavy metals, mycotoxins, and environmental chemicals. In my experience, toxic burden is more common than most patients anticipate — and more clinically significant in the context of rosacea than it is typically given credit for.
Why Rosacea Gets Worse in Perimenopause
Perimenopause is not simply a hormonal transition. It is a systemic shift toward a pro-inflammatory, insulin-resistant state — and that shift creates the precise internal environment in which rosacea thrives.
Here is what’s happening physiologically:
- Declining progesterone creates relative estrogen dominance, directly stimulating mast cell activity and histamine output.
- Estrogen fluctuations during the transition (before the eventual decline of late perimenopause and menopause) can trigger unpredictable mast cell degranulation and histamine surges — explaining why many women notice flares that seem random and unrelated to obvious triggers.
- Increasing insulin resistance impairs blood sugar regulation, driving endothelial damage, angiogenesis, and vascular instability in the skin.
- Gut permeability increases as estrogen and progesterone decline, reducing the integrity of tight junctions in the intestinal wall and impairing DAO enzyme production.
- The gut microbiome undergoes significant changes — including reduced diversity and shifts in the estrobolome — that worsen estrogen metabolism and amplify systemic inflammation.
- The body moves into a pro-inflammatory cytokine state that is inherently more reactive, lowering the threshold at which ordinary stimuli produce an exaggerated skin response.
The result: women who had manageable rosacea in their 30s often find it accelerating significantly in their 40s and beyond. And women who had no history of rosacea sometimes develop it for the first time during perimenopause — and don’t understand why.
This is not a coincidence. It is a predictable consequence of the systemic changes of perimenopause on an inflammatory skin condition with internal roots. And it is almost never addressed in the conventional dermatology model.
Testing: What I Look For and Why
While every workup is tailored to the individual, the following panels give me the most clinically meaningful picture in rosacea cases — and here’s why each one matters.
Vibrant Wellness Hormone Zoomer
Full assessment of estrogen, progesterone, testosterone, cortisol, and estrogen metabolism. I am looking specifically for estrogen dominance patterns — either high estrogen relative to progesterone, poor estrogen clearance through Phase I and Phase II liver detoxification, or both. This is the single most consistently revealing panel in rosacea cases.
Comprehensive Food Sensitivity Panel
IgG and IgA-mediated food sensitivity testing. Because food sensitivities are often a chronic, silent driver of immune activation — contributing to blood sugar dysregulation, endothelial damage, gut permeability, and mood imbalances — identifying and removing reactive foods is frequently one of the highest-impact initial interventions.
Gut Zoomer
Comprehensive stool analysis assessing microbiome composition, pathogenic organisms, inflammatory markers, DAO production markers, and digestive function. Critical for understanding the gut-skin connection and the health of the estrobolome.
Total Tox Burden
Heavy metals, mycotoxins, and environmental chemicals. Mast cell activation, impaired estrogen clearance, and histamine accumulation all worsen with toxic burden, making this an essential part of a complete rosacea assessment.
Micronutrient Panel with SNPs
Assesses cellular levels of vitamins, minerals, amino acids, and antioxidants — along with genetic variants that affect nutrient metabolism. Deficiencies in key nutrients (including those required for histamine breakdown, liver detoxification, and skin barrier integrity) are common and directly relevant to rosacea management.
Standard Metabolic Markers
Fasting insulin, HbA1C, full thyroid panel, CMP, lipid panel, and liver enzymes. Blood sugar regulation, thyroid function, and liver health are foundational to the hormonal and inflammatory picture.
The Functional Medicine Approach: Internal and Topical
Every protocol I build is individualized to what the testing reveals. That said, there are core clinical priorities that apply consistently in rosacea cases — both from the inside out and the outside in.
Internal Support
The interventions I reach for most consistently in rosacea cases include the following — though the full protocol is always built around what your health history, symptoms and specific testing reveals:
- Omega3 BioPure — Omega-3 fatty acids are foundational for skin health at the cellular level: they contribute to phospholipid bilayer formation, support the acid mantle, reduce trans-epidermal water loss, and have a direct anti-inflammatory effect on mast cell activity and vascular reactivity.
- BioC (Vitamin C with Bioflavonoids) — Vitamin C is a natural antihistamine that helps to reduce histamine release from mast cells. The bioflavonoids further support vascular integrity, which is directly relevant to the capillary instability visible in rosacea.
- GI-MaxAid — Supports leaky gut repair and restoration of the intestinal lining. A healthy gut lining is required for adequate DAO enzyme production — the primary enzyme responsible for histamine degradation in the gut. Without it, histamine accumulates.
- Methylated B-Complex — B vitamins are required cofactors for systemic histamine breakdown (particularly B6 and B12 in the DAO and HNMT enzyme pathways), estrogen metabolism through both Phase I and Phase II liver detoxification, and stress hormone and toxin clearance. Methylated forms are essential for women with MTHFR variants, which are common.
These are broad clinical anchors. The full supplement protocol is always customized to the individual based on testing, health history, symptoms and clinical pattern.
Topical Support: Restoring the Skin Barrier
The topical approach in rosacea prioritizes barrier restoration, structural integrity, and reduction of vascular reactivity — not suppression. The skin of a rosacea patient is typically sensitized, barrier-compromised, and lacking in the foundational nutrients needed to rebuild resilience. Topical support is equally individualized, but the clinical priorities remain consistent across most rosacea cases:
- Vitamin A — Non-negotiable in rosacea. Vitamin A normalizes cell turnover, reduces inflammatory signaling in the skin, supports collagen and elastin production, and helps restore the structural integrity of the dermis and epidermis. It must be introduced gradually and at the right concentration for sensitized skin.
- Vitamin C — Paired with Vitamin A for collagen synthesis, antioxidant protection, and capillary strengthening. Works synergistically with oral BioC.
- Broad-spectrum SPF — UV exposure is one of the most reliable triggers of mast cell activation. Consistent SPF is non-negotiable in rosacea management.
My current Environ recommendations for rosacea-prone skin include the Pre-Cleansing Oil, Vita-Enriched Antioxidant Gel, AVST 1 Moisturizer, Anti-Pollution Spritz, and Tizo or RAD SPF. The emphasis is always on gradual vitamin A introduction and barrier support before any more active intervention. All skincare recommendations are customized.
A Patient Story
One of my clients came to me having managed rosacea for most of her adult life — primarily with oral and topical antibiotics. She had seen multiple dermatologists. She was meticulous about trigger avoidance. And her rosacea continued to worsen.
She also had high blood pressure, acid reflux, bloating, and anxiety — symptoms she viewed as completely unrelated to her skin. In my intake assessment, I saw a different picture: a pattern of interconnected dysfunction with a common upstream driver.
Through functional medicine testing and a comprehensive health history, we identified the root causes specific to her case and built an individualized protocol that addressed them systemically. In less than four months, her rosacea had cleared significantly. Her blood pressure normalized — without medication. The acid reflux and bloating resolved. Her anxiety improved markedly. She lost 12 pounds as an unexpected side effect of reduced inflammation and improved metabolic function.
She was surprised that conditions she had treated separately for years were all expressions of the same underlying imbalance. That interconnectedness is exactly what functional medicine is designed to see.
Frequently Asked Questions About Rosacea
Q1: What is the root cause of rosacea?
Rosacea is driven by immune dysregulation and internal inflammatory triggers — most commonly mast cell activation, histamine overload, estrogen dominance, food sensitivities, blood sugar dysregulation, gut dysbiosis, and toxic burden. These drivers are interconnected and tend to compound one another. Functional medicine identifies which combination is active in your specific case rather than managing surface-level symptoms.
Q2: Why does rosacea get worse during perimenopause?
Perimenopause creates a systemic shift toward a pro-inflammatory, insulin-resistant state. Declining progesterone leads to relative estrogen dominance, which directly stimulates mast cells and increases histamine. Increasing insulin resistance drives vascular damage and angiogenesis. Gut permeability increases, impairing histamine breakdown and estrogen clearance. Together, these changes amplify every underlying driver of rosacea.
Q3: What is the connection between histamine and rosacea?
Histamine is released by mast cells in the skin in response to inflammatory triggers, causing vascular dilation, flushing, and redness. When histamine is produced faster than the body can break it down — due to impaired DAO enzyme production, poor liver clearance, or chronic mast cell activation — it accumulates and drives persistent rosacea symptoms. Addressing the upstream drivers of mast cell activation and supporting histamine breakdown are key functional medicine targets.
Q4: Can food sensitivities cause rosacea flares?
Yes — and they are one of the most frequently overlooked drivers. Food sensitivities create a chronic, low-grade immune activation that releases stress hormones, elevates blood sugar, damages endothelial lining, and promotes angiogenesis and vascular reactivity in the skin. Because reactions are often delayed 24–72 hours, patients rarely connect specific foods to their flares without systematic testing.
Q5: What does functional medicine testing for rosacea look at?
A comprehensive functional medicine rosacea workup typically includes hormonal assessment (Hormone Zoomer), comprehensive food sensitivity testing, gut microbiome analysis (Gut Zoomer), total toxic burden screening (Total Tox), micronutrient testing with SNPs, and standard metabolic markers including fasting insulin, fasting blood glucose, HbA1C, full thyroid panel, lipid panel and liver enzymes. Together, these panels map the full internal picture driving inflammation.
Q6: Is rosacea linked to gut health?
Strongly. Leaky gut allows bacterial fragments (LPS) into the bloodstream, triggering systemic immune activation. Gut dysbiosis impairs DAO enzyme production needed to break down histamine. A disrupted estrobolome worsens estrogen dominance. All of these mechanisms directly drive or amplify rosacea. Gut restoration is a core component of functional medicine rosacea treatment.
Q7: Can I permanently get rid of rosacea?
Rosacea can go into long-term remission — and for many of my patients, it clears significantly and stays clear — but whether that constitutes “permanent” depends on whether the underlying drivers are fully identified and addressed. When mast cell activation, histamine overload, estrogen dominance, gut dysbiosis, food sensitivities, and toxic burden are resolved systematically, the inflammatory conditions that sustain rosacea are no longer present. The skin reflects that. Trigger avoidance and antibiotics manage symptoms without resolving those drivers, which is why flares keep returning. A root-cause functional medicine approach aims for lasting resolution, not ongoing management.
Q8: What organ causes rosacea?
Rosacea is not caused by a single organ — it is a systemic inflammatory condition with multiple internal drivers. In functional medicine, we consistently find the gut, liver, endocrine and immune system at the center of the picture. The gut drives rosacea through dysbiosis, leaky gut, impaired histamine breakdown, and disrupted estrogen metabolism. The liver contributes through poor estrogen clearance and impaired detoxification. The immune system — specifically mast cell activation and chronic inflammatory signaling — is the mechanism through which these upstream imbalances express themselves on the skin. Rosacea shows up on the face, but it originates much deeper.
Q9: Why have I suddenly developed rosacea?
Rosacea rarely appears truly out of nowhere — what looks sudden is usually the tipping point of multiple internal drivers that have been building quietly. The most common triggers I see clinically are hormonal shifts (particularly the transition into perimenopause, which creates relative estrogen dominance and a pro-inflammatory state), a significant increase in toxic burden, a gut disruption such as dysbiosis or leaky gut, or the accumulation of unidentified food sensitivities reaching a threshold where the immune system can no longer compensate. Stress, antibiotic use, and dietary changes can also shift the internal environment enough to tip a subclinical pattern into visible rosacea. The question worth asking is not just “why now” but “what has changed internally.”
Q10: What is the best treatment for rosacea?
The most effective approach to rosacea is one that identifies and addresses your specific internal drivers rather than managing surface symptoms. Antibiotics, topical prescriptions, and trigger avoidance can quiet flares temporarily, but they do not resolve the mast cell activation, histamine overload, estrogen dominance, gut dysbiosis, food sensitivities, toxic burden, or other upstream drivers that sustain the condition. In my functional medicine and functional dermatology practice, the best treatment is always individualized — built around your health and medical history, symptoms that you’re experiencing, comprehensive testing and the specific pattern driving your rosacea. Both internal support and topical barrier restoration are part of the protocol, and everything is tailored to your unique case
Q11: Why does my rosacea keep coming back?
Recurring rosacea is almost always a sign that the upstream internal drivers have not been identified or addressed. Conventional treatment — antibiotics, topical prescriptions, trigger avoidance — manages visible symptoms without correcting the mast cell activation, histamine overload, gut dysbiosis, estrogen dominance, thyroid dysfunction, Demodex overgrowth, blood sugar dysregulation, or nutrient insufficiency producing them. When treatment ends, the internal environment reasserts itself and flares return — often with increasing frequency or severity over time. Lasting resolution requires identifying your specific upstream drivers through comprehensive testing and addressing them systematically. The goal is not ongoing management of a chronic condition. It is correcting the intern
Q12: Why didn’t antibiotics help my rosacea?
Because antibiotics address one visible aspect of rosacea — inflammatory papules and pustules — without investigating or correcting any of the upstream drivers producing them. Mast cell activation, histamine overload, gut dysbiosis, poor estrogen clearance, thyroid dysfunction, blood sugar dysregulation, Demodex overgrowth, and food sensitivities are all common rosacea drivers that antibiotics do not touch. Long-term antibiotic use also depletes the gut microbiome, impairs DAO enzyme production needed for histamine breakdown, reduces B vitamin status affecting methylation and immune function, and worsens intestinal permeability — paradoxically amplifying several of the upstream drivers it was meant to address. If antibiotics produced some improvement that did not last, the antibiotic was managing a downstream symptom. If they produced no improvement at all, the primary drivers in your case are likely not bacterial in the conventional sense and require a different investigative framework entirely.
Ready to Address the Root Cause?
If you’ve been managing rosacea with conventional treatment and continuing to flare, the missing piece is almost certainly internal. The question isn’t what to put on your skin — it’s what’s driving the inflammation that keeps showing up there.
The functional medicine approach to rosacea does not rely on antibiotics or prescriptions. It relies on identifying what is specifically driving inflammation in your body — and addressing those drivers directly. For many women, this means meaningful, lasting improvement where conventional treatment has repeatedly fallen short.
This is the foundation of my functional dermatology approach to rosacea — identifying and addressing the internal drivers that conventional dermatology doesn’t investigate.
I offer virtual Initial Functional Medicine Health and Skin Assessments for women who are ready to look upstream. This is where we take a full picture of your health history, your current symptoms, and the patterns that connect them — and build a testing and protocol strategy specific to your body.
→ Book your Initial Functional Medicine Health and Skin Assessment
Written by Natalie Maibenko – a Certified Functional Medicine Practitioner and Master Esthetician with 22+ years of experience and founder of Unique Verve

As a Certified Functional Medicine Practitioner my Expertise Encompasses:
- Immune System: frequent illness, UTIs, yeast infections
- Allergies, Asthma
- Skin Problems: acne, cystic acne, rosacea, eczema, dermatitis, ichthyosis, psoriasis, vitiligo, melasma
- Inflammation: arthritis, rhinitis, joint & muscle pain, migraines, headaches
- Sleep Disturbunces, Insomnia
- Gut Problems: IBS/IBD, bloating, acid reflux, gas, constipation, diarrhea, parasites, fungal/yeast overgrowths
- Hormonal Imbalances: PCOS, PMS symptoms, weight problems/inability to lose weight, thyroid problems
- Hair Loss, Alopecia
- Mood Imbalances: anxiety, depression, irritability
- Metabolic Dysfunction, Insulin Resistance, Type 2 Diabetes
- Optimizing Wellness for Successful Pregnancy
- Autoimmune Conditions: Hashimoto’s thyroiditis, grave’s disease, reumatoid arthritis (RA), lupus, etc
- Bone Health: osteopenia/ osteoporosis
- Effective Anti-Aging Strategies without Injectables with the inside-out & outside-in approach
- Detoxification of Heavy Metals, Mycotoxins, Environmental Toxins
- Reversing Breast Implant Illness
- Preparation for the Explant Surgery and Optimization of Wellness & Vitality Post-Explant
With love and gratitude,
Natalie Maibenko
Functional Medicine & Skincare Expert – Helping You Take Control of Your Health and Achieve Lasting Skin Results
Disclaimer: Information and content on this website is provided for educational purposes only, and is not intended to diagnose, treat and to be a substitute for the advice provided by your physician or other healthcare professional. No information offered here should be interpreted as a diagnosis of any disease, nor an attempt to treat or prevent or cure any disease or condition. If you have any concerns or questions about your health, you should always consult with a physician or other healthcare professional. Do not disregard, avoid, or delay obtaining medical or health-related advice from your healthcare professional. Always speak with your healthcare professional before taking any medications, supplements or pursuing any wellness programs. Information provided on this website does not create a doctor-patient relationship between you and any professional affiliated with this website.