If you’ve been prescribed spironolactone for acne — or you’re on it right now and still breaking out — this post is for you. We’re going to talk about what this drug actually does inside your body, why it works for some women and not others, and why stopping it can send your skin into a tailspin. More importantly, we’re going to talk about what’s actually driving your acne — and why that answer almost never comes up in a dermatology appointment.
First, Let’s Be Honest About What Spironolactone Is
Spironolactone — often called “spiro” — is a blood pressure and heart medication that dermatologists have been prescribing off-label for hormonal acne in women for decades. It works by blocking androgen receptors and suppressing the androgens (male hormones like testosterone and DHT) that trigger excess oil production in the skin. Less oil, fewer clogged pores, fewer breakouts. The logic is sound, and for many women, it does provide real relief.

But here’s what that relief actually is: a triage. A way to quiet a symptom while the underlying problem continues, unaddressed, beneath the surface.
This isn’t a criticism of the women who take it or the doctors who prescribe it. Hormonal acne is painful, persistent, and emotionally exhausting — and sometimes you need something to stop the bleeding while you figure out what’s actually wrong. The concern is what happens when the triage becomes the treatment plan, and the deeper questions never get asked.
Why Your Androgens Are Elevated in the First Place
Spironolactone suppresses androgen activity. But it doesn’t ask — or answer — the question of why your androgens were elevated to begin with.
In a functional medicine context, elevated androgens in women are almost never a standalone problem. They’re downstream of something else. The most common upstream drivers include:
Blood sugar dysregulation and insulin resistance. When blood sugar runs high and insulin output spikes in response, the ovaries get a signal to produce more androgens. This is one of the most underrecognized drivers of hormonal acne in women — and it’s directly connected to diet. A pattern high in refined carbohydrates, processed foods, and sugar creates a cycle of blood sugar spikes and insulin surges that continuously feeds androgen excess. This is also why acne and PCOS are so closely linked — insulin resistance is central to both.
Chronic stress and HPA axis dysregulation. The hypothalamic-pituitary-adrenal-thyroid-gonadal (HPATG) axis is the body’s stress response system, and it doesn’t distinguish between emotional stress, physical stress, and physiological stress. A demanding job, a significant loss, chronic sleep deprivation, gut inflammation, or exposure to environmental toxins — all of these send stress signals that drive cortisol production, which in turn drives androgen production. Over time, this chronic activation can lead to adrenal dysregulation and, downstream, thyroid suppression.
Endocrine-disrupting compounds. Plastics, pesticides, mold toxins (mycotoxins), heavy metals, and other environmental compounds can directly interfere with hormone production, metabolism, and clearance. When these compounds accumulate, they act as physiological stressors that dysregulate blood sugar, impair liver detoxification of hormones, and contribute to androgen excess — all without ever showing up on a standard blood panel.
Gut dysbiosis and intestinal permeability. The gut and gut health is deeply involved in hormone regulation, particularly estrogen metabolism. When gut health is compromised, endotoxins (LPS) from bacteria can enter systemic circulation, creating low-grade inflammation that further disrupts hormone balance and drives acne from the inside.
Post-birth control rebound. This is a pattern worth naming specifically because it’s extremely common. Many women are prescribed spironolactone after stopping hormonal birth control — because stopping the pill can trigger a significant rebound in androgen activity that the pill had been suppressing. The spironolactone then continues the suppression. But neither medication has addressed what the hormonal environment actually looks like without pharmaceutical intervention, or why it defaults to androgen excess.
The pattern I see repeatedly in practice: a woman in her twenties, thirties, or forties — the age range for spironolactone patients is wide — who has been managing her hormones with one medication or another for years, often without anyone running a comprehensive hormone panel, checking insulin, or asking about her stress levels, diet, or environmental exposures.
What Spironolactone Is Doing to the Rest of Your Body
Every drug has consequences on other systems in the body. Spironolactone is no exception — and some of its systemic effects are directly relevant to the women taking it for skin reasons.
It’s a diuretic — and that matters for your skin
Spironolactone works by reducing aldosterone, which causes the kidneys to excrete more sodium and water. This is why some women lose a bit of water weight when they start taking it. But chronic diuretic action has consequences, including one that’s rarely discussed in a dermatology context: it can impair enzyme function in the skin.
Enzymes in the epidermis depend on adequate free water to work properly. When the skin becomes chronically dehydrated from the inside — not just from external weather or product choices, but from systemic fluid loss — enzyme activity slows. Slower enzyme activity means impaired desquamation: the natural process by which dead skin cells shed from the surface. When dead skin cells accumulate instead of shedding normally, they contribute to congestion, uneven texture, and — over time — acne formation.
This is one of the mechanisms behind the rebound acne many women experience when they stop spironolactone. The drug suppressed the androgenic trigger for oil production, but it may have simultaneously impaired the skin’s own renewal process. When the drug is removed, both problems surface at once.
It Can Trigger a Chain of Events That Depletes Magnesium — In Some Women
To be precise: spironolactone is not a direct magnesium-wasting drug. It is potassium and magnesium sparing by its primary mechanism of action. However, in some women, it sets off an indirect chain of events that can result in meaningful magnesium insufficiency — and understanding that chain matters clinically.
Spironolactone is more commonly associated with diarrhea than constipation. For some women, this gastrointestinal side effect is mild and transient. But when diarrhea is sustained, the consequences compound quickly. Rapid intestinal transit time prevents adequate absorption of magnesium in the gut, leading to progressive magnesium loss through stool. Chronic gastrointestinal disturbance is in fact one of the primary mechanisms of magnesium deficiency — and it doesn’t require dramatic symptoms to be clinically significant.
This creates a paradoxical situation that some women on spironolactone find themselves in without ever connecting the dots: the drug triggers diarrhea, diarrhea impairs magnesium absorption, magnesium insufficiency disrupts gut motility over time — and some of those women then develop constipation, the very opposite symptom, as a downstream consequence of the mineral loss and its effect on smooth muscle function in the bowel.
The gastrointestinal disruption doesn’t stop at magnesium. Sustained diarrhea impairs the absorption of other essential minerals and fat-soluble vitamins — including zinc and vitamin A, two of the most critical nutrients for acne prevention and control. Zinc is essential for regulating sebum production, supporting skin immune function, and modulating androgen activity at the receptor level. Vitamin A is the primary regulator of sebaceous glands, skin cell turnover, keratinization, and follicular health. When both are depleted — whether through poor absorption, genetic impairment, insufficient intake or a combination of both — the skin loses two of its most important internal defenses against acne formation.
This is another mechanism through which some women experience no real improvement in acne while taking spironolactone, or a strong rebound when they stop: the drug may have been simultaneously depleting the very nutrients their skin needed to heal.
It bears repeating that this is not a universal effect. Not every woman on spironolactone will develop diarrhea, and not every woman who develops diarrhea will progress to magnesium or fat-soluble vitamin insufficiency. But for women who are experiencing gastrointestinal symptoms on spironolactone — whether diarrhea, cramping, or what feels like a later shift toward constipation — this chain of events is worth taking seriously. In my functional medicine practice I use Vibrant Wellness Micronutrient panel with SNPs which is the most precise way to identify whether these depletions are present and how genetically predisposed a given individual is to them.
As with every mechanism discussed in this post, the underlying principle holds: every drug has consequences on other systems in the body. Some of those consequences are direct. Others, like this one, are indirect — but no less real, and no less worth finding and fixing.
It can contribute to adrenal suppression — especially in women who are already depleted
This is the clinical concern I want every woman on long-term spironolactone to understand. If you are already experiencing low energy, apathy, lethargy, difficulty getting through the day, or low motivation — these can be signs of adrenal dysregulation. Spironolactone’s effect on aldosterone (an adrenal hormone) means that long-term use, particularly in someone whose adrenal function is already compromised, can push the HPA axis further toward under-reactivity.
A hypo-reactive HPA axis then contributes to low thyroid function — because the two systems are closely connected. And low thyroid function worsens acne, affects mood, disrupts metabolism, and contributes to fatigue. The cruel irony is that when a woman finally stops spironolactone, the acne comes back — but now there’s also a depleted adrenal-thyroid picture underneath it that wasn’t there, or wasn’t as pronounced, when she started.
The nutrient depletion problem is compounded by genetics
When we run a Micronutrient panel with SNPs (single nucleotide polymorphisms — genetic variants that affect how your body absorbs and uses nutrients), we frequently find that women on spironolactone who are struggling with persistent symptoms already have genetic impairments in the very nutrients that protect against acne. Vitamin A and zinc are two of the most important for skin health, and both are commonly affected by SNPs that reduce absorption or utilization. If you have a genetic predisposition to low vitamin A or zinc, and spironolactone is further depleting your nutritional reserves, you’re facing a double challenge that no topical retinoid or prescription drug will fix.
What Testing Actually Reveals
Standard dermatology workups for acne are typically minimal — a visual assessment, maybe a referral for basic hormones. In a functional medicine approach, the testing picture looks very different, and for good reason: we’re trying to understand the full chain of causation, not just the end result on the skin.
When working with women who have hormonal acne — particularly those on or coming off spironolactone — here’s the testing framework:
Comprehensive Metabolic Panel (CMP): Gives us a window into electrolyte balance (sodium, potassium, calcium), kidney function, and hydration status. In women on spironolactone, we sometimes see a skewing of sodium and potassium levels that confirms the adrenal picture. We also look at other markers such as albumin and total protein as markers of hydration — values that can confirm whether the diuretic action of the drug is contributing to systemic dehydration.
Fasting insulin, fasting glucose, and HbA1c: These three together tell us whether blood sugar dysregulation is a driver. Elevated fasting insulin is often the earliest sign of insulin resistance — and it can be present even when fasting glucose looks normal. This is critical because insulin resistance is one of the most common upstream causes of androgen excess and hormonal acne.
Full lipid panel: Beyond cardiovascular risk, the lipid panel gives useful functional clues. Elevated LDL and total cholesterol can indicate sluggish thyroid function. Low HDL can point to oxidative stress. Elevated triglycerides indicate metabolic dysregulation — a direct driver of hormonal imbalance and acne.
Full thyroid panel: TSH alone is not enough. We look at free T3, free T4, reverse T3, and thyroid antibodies. As discussed, chronic stress and adrenal dysregulation suppress thyroid function, and thyroid dysfunction worsens acne. This connection is rarely made in conventional care.
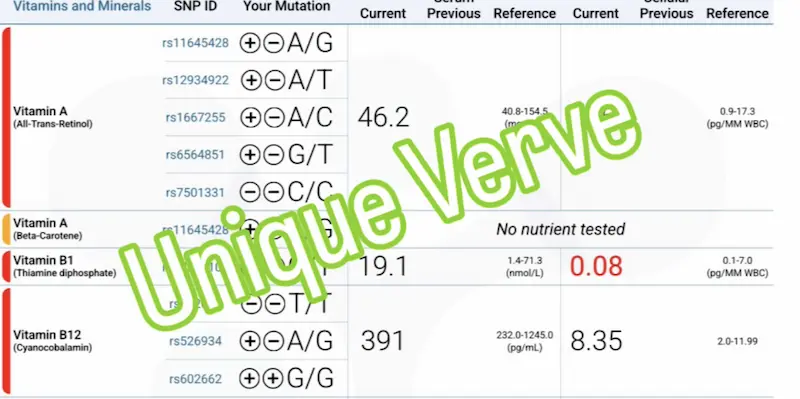
Micronutrient panel with SNPs (Vibrant Wellness): This is one of the most informative tests in our acne workup. It shows us not just what nutrients are low or suboptimal, but why — by identifying genetic variants that impair absorption or utilization. We look specifically at vitamin A, vitamin D, zinc, all B vitamins (for methylation and detoxification capacity), and omega-3 status. The combination of low nutrient levels and unfavorable SNPs tells us exactly where supplementation needs to be targeted — and why a generic multivitamin isn’t going to move the needle.
Vibrant Comprehensive Urinary Hormone Panel: This is where the hormone picture becomes truly clear — and it’s very different from what a standard serum hormone panel shows. Urinary hormone testing measures not just circulating hormones, but their metabolites: what the body is doing with those hormones, which pathways it’s preferring, and where the process is breaking down. In women with hormonal acne, I commonly see elevated androsterone and etiocholanolone (androgen metabolites), elevated DHT, and a preference for 5-alpha reductase activity — meaning the body is converting hormones preferentially into the most potent, acne-driving androgens.
Total Tox Burden (Vibrant Wellness): When the hormone panel or symptom picture suggests significant environmental load — and particularly when mycotoxins, heavy metals, or endocrine disruptors are suspected — this panel can provide additional insights to hormone dysregulation. Mycotoxins (mold toxins) are surprisingly common in acne cases, particularly in women who have lived or worked in water-damaged buildings. They act as powerful physiological stressors, driving blood sugar up, impairing liver detoxification, and contributing to hormone dysregulation. Heavy metals and endocrine-disrupting compounds (EDCs) compound this effect. Finding an elevated toxic burden explains why some women do everything right with diet and lifestyle and still can’t clear their skin.
A Real Patient Story
A woman in her early twenties came to see me while already four months into spironolactone — with no improvement in her skin. She was also taking naproxen (an NSAID) for one week each month to manage severe PMS, and an antihistamine daily for allergies. Before spironolactone, she’d tried multiple rounds of antibiotics without lasting results.
Acne wasn’t actually her primary concern. She came in because of a constellation of other symptoms that were significantly affecting her quality of life: depression, anxiety, intense sugar and carbohydrate cravings, bloating, constipation, lethargy, fatigue, muscle and joint pain, terrible PMS, chronic allergies, and sinus issues.
Testing told a detailed story. Her fasting insulin was 60.5 (reference range: 2.6–24.9) — significant insulin resistance. Some of the markers on CMP test showed evidence of dehydration — almost certainly compounded by spironolactone’s diuretic effect. Her lipid panel showed elevated cholesterol and LDL.
Her Micronutrient panel with SNPs revealed low vitamin A with a double genetic impairment in vitamin A utilization; low vitamin D3 with double SNPs; genetic variants affecting all B vitamins, impairing methylation and detoxification capacity; a double SNP affecting zinc; a high arachidonic acid to EPA ratio; and a low omega-3 index. Her Total Tox Burden confirmed elevated mycotoxins, heavy metals, and endocrine disruptors — consistent with the methylation and detox impairment her SNPs predicted. Her urinary hormone panel showed 5-alpha reductase dominance with poor estrogen phase 2 clearance and a phase 1 preference toward the 16-OH and 4-OH pathways (these are DNA damaging pathways that can lead to cancer development).
Every one of her symptoms — the depression, the anxiety, the fatigue, the cravings, the PMS, the gut issues, the joint pain, the acne — was connected. The testing didn’t reveal ten separate problems. It revealed one interconnected picture with a coherent root cause.
After three months of a personalized functional medicine program — combining targeted supplementation based on her health history, symptoms and test results, dietary and lifestyle interventions, and customized Environ skincare — her acne was gone, and so were all of her other symptoms. She no longer takes any medications.
The Skincare Side of the Equation
Internal work is primary, but topical care matters — and in the context of spironolactone-related skin changes, the approach needs to be calibrated carefully.

The most important shift: I treat all acne patients as sensitive skin first. This runs counter to the conventional dermatology approach of loading acne-prone skin with strong actives — benzoyl peroxide, high-concentration AHAs and BHAs, aggressive retinoids — which can strip and compromise the skin barrier, worsen dehydration already present from spironolactone’s diuretic action, and trigger reactive oil production.
The foundational principles of the topical protocol I build for each patient are consistent, even when the specific products differ:
A gentle oil-based first cleanse from Environ Skincare that emulsifies with water, removes sunscreen and makeup effectively, and supports barrier function without stripping. For congested, acne-prone skin, oil cleansing is often counterintuitive — but clinically it is one of the most important first steps in reestablishing a healthy skin environment.
Environ Vitamin A, C, E, and beta-carotene based moisturizers to normalize skin cell function, regulate oil production, support cell turnover, and aid in healing. Vitamin A is the most critical nutrient for skin normalization — it regulates keratinization, reduces sebum production, and supports the immune function of the skin. This is particularly important when testing has confirmed genetic impairments in vitamin A utilization.
Targeted support for active lesions, calibrated to the severity of existing acne and adjusted as the skin responds and heals.
Barrier-reparative and soothing support for skin that has been under chronic stress — from hormonal dysregulation, medication side effects, or prior overly aggressive skincare.
Climate and environment inform every product selection. A dry winter climate in Boston and a humid coastal environment in Florida require fundamentally different approaches — particularly around the use of exfoliating acids, which affect enzyme activity in the skin differently depending on ambient humidity levels.
All skincare recommendations at Unique Verve are made within the context of a full skin and health assessment — never as a one-size-fits-all prescription. If you are ready to find out which Environ products are right for your specific skin, that conversation begins with your Comprehensive Health History and Skin Health Assessment. You can also browse the full Environ skincare collection available through our shop.
What the Path Forward Looks Like
Coming off spironolactone — when that’s the right decision, made in consultation with your prescribing provider — isn’t something to do abruptly. Tapering is important, and it works best when the internal work through functional medicine is already underway: when blood sugar is stabilizing, when the nutrient depletions are being corrected, when the hormone metabolism picture is shifting.
The functional medicine process begins with a comprehensive assessment: a detailed health history, a full symptom review, and a skin assessment that considers both internal and topical factors together. From there, testing is ordered based on what the clinical picture suggests — not as a standard panel applied to everyone, but as a targeted investigation of the specific drivers most likely at play for this individual.
The goal is never to tell a patient what to do with her medications. That conversation belongs with the prescribing provider. The goal is to understand what’s actually driving her acne, correct the underlying imbalances, and support her skin — and her body — in a way that doesn’t require ongoing pharmaceutical suppression.
A Note on SSRIs and Acne
One pattern worth mentioning — though it deserves its own dedicated post — is the connection between SSRI antidepressants and acne. SSRIs are metabolized by the liver and can, in some women, contribute to liver overwhelm that impairs the metabolism of sex hormones and stress hormones. They have also been shown to promote intestinal permeability (leaky gut), gut dysbiosis, increasing the bacterial endotoxin load (LPS) that drives systemic inflammation — and, with it, acne. The nutrient depletion that follows from impaired gut absorption creates a cycle that’s difficult to break without addressing the root cause.
In my functional medicine practice, it is actually very common to see women who are taking both spironolactone and an SSRI simultaneously. This combination makes complete sense when you understand the clinical picture: the same upstream drivers that dysregulate hormones and trigger acne — chronic stress, blood sugar imbalance, gut dysfunction, nutrient depletion — are often the same drivers that contribute to anxiety and depression. These are not separate problems. They are different expressions of the same underlying systemic imbalance.
I work with these women regularly. Having multiple medications on board does not disqualify you from a functional medicine approach — it makes the case for one stronger. Understanding how each medication is affecting your body, what it may be depleting, and what the deeper picture looks like underneath both prescriptions is exactly the kind of work we do together in the Comprehensive Health History and Skin Health Assessment. If you are on an SSRI and spironolactone and your skin — or your health more broadly — is still not where you want it to be, you are not out of options. You are simply missing a deeper layer of the answer.
What I Want You to Walk Away Understanding
Spironolactone gives your skin a break. For some women, that break is exactly what’s needed while they address the deeper picture. For others, it’s a detour that delays the real work by months or years — sometimes at the cost of adrenal reserve, thyroid function, and nutritional status that were already under strain.
Your acne is not a cosmetic problem. It is a signal from your body that something in the internal environment is dysregulated — hormonally, metabolically, nutritionally. The fact that a drug can quiet that signal doesn’t mean the signal wasn’t worth hearing.
Every medication has consequences on other systems in the body. Asking what those consequences are — and what was driving the problem in the first place — is not a radical question. It’s the question that leads to actually getting better.
Ready to Find Your Root Cause?
Your acne may be what brought you here — but if you’ve been reading this post and recognizing yourself in the fatigue, the mood shifts, the bloating, the PMS, the brain fog, the sugar cravings, or the feeling that something deeper is simply off — that recognition matters. These are not separate problems. They are one interconnected picture, and they all deserve answers.
The process begins with a Comprehensive Health History and Skin Health Assessment — a virtual appointment where we map your full symptom picture, not just your skin. We look at everything: your hormones, your metabolism, your gut health, your stress load, your medications, your nutrient status, and your history. From there we build a personalized testing and treatment plan designed to address the root cause of all of it — not just the breakouts.
If you are ready to stop managing symptoms one by one and start understanding what is actually driving them, this is where that conversation begins.
Book your Comprehensive Health History and Skin Health Assessment →
Frequently Asked Questions About Spironolactone For Acne
Does spironolactone permanently fix hormonal acne?
No. Spironolactone manages hormonal acne by suppressing androgen activity, but it does not address why androgens are elevated in the first place. The most common upstream drivers — insulin resistance, chronic stress, poor hormone clearance, nutrient depletion, and environmental toxin burden — continue untreated while the drug is active. For most women, acne returns when spironolactone is stopped because the root cause was never identified or corrected.
Why does acne come back worse after stopping spironolactone?
Rebound acne after stopping spironolactone happens through two simultaneous mechanisms. First, the internal imbalances driving androgen excess — such as insulin resistance, adrenal dysregulation, or impaired hormone metabolism — resurface immediately because they were never treated. Second, spironolactone’s diuretic action can impair enzyme activity in the skin over time by causing chronic dehydration, which disrupts the natural shedding of dead skin cells. When both factors emerge at once after stopping the drug, the rebound can be more severe than the original acne.
What does spironolactone do to your hormones long-term?
Beyond suppressing androgen activity, long-term spironolactone use can deplete magnesium — an essential mineral for stress hormone metabolism, estrogen clearance, gut motility, and cellular energy production. It can also contribute to adrenal suppression, particularly in women who are already experiencing fatigue, low energy, or high stress loads. Adrenal dysregulation in turn can suppress thyroid function, creating a downstream hormonal picture that may not become fully apparent until the medication is stopped.
What are the most important labs to run for hormonal acne?
A comprehensive functional medicine workup for hormonal acne goes well beyond standard hormone levels. Key panels include a Comprehensive Metabolic Panel (CMP) for electrolytes, kidney function, and hydration status; fasting insulin, fasting glucose, and HbA1c to assess metabolic drivers; a full lipid panel for thyroid and oxidative stress clues; a complete thyroid panel including free T3, free T4, reverse T3, and antibodies; a Micronutrient panel with SNPs to identify nutrient deficiencies and genetic impairments; and a comprehensive urinary hormone panel to evaluate androgen metabolites and estrogen clearance pathways. A Total Tox Burden panel may also be indicated when mycotoxins, heavy metals, or endocrine disruptors are suspected.
What causes elevated androgens in women with acne?
Elevated androgens in women with hormonal acne are almost always downstream of other imbalances rather than a primary hormone disorder. The most common drivers are blood sugar dysregulation and insulin resistance — which signal the ovaries to overproduce androgens — alongside chronic stress and HPA axis dysregulation, impaired liver detoxification of sex hormones, gut dysbiosis, and exposure to endocrine-disrupting compounds such as mycotoxins, heavy metals, and environmental chemicals. Treating the androgen elevation directly with spironolactone without addressing these upstream causes is why hormonal acne so frequently returns.
Can spironolactone affect adrenal and thyroid function?
Yes, particularly with long-term use. Spironolactone works by reducing aldosterone, an adrenal hormone. In women who are already experiencing adrenal stress — reflected in symptoms like low energy, fatigue, apathy, and poor stress tolerance — chronic aldosterone suppression can contribute to a further under-reactive HPA axis. This matters because adrenal dysregulation is closely linked to thyroid suppression, and low thyroid function worsens acne, affects mood, slows metabolism, and contributes to fatigue. These connections are rarely discussed in a dermatology context but are clinically significant.
Does spironolactone deplete magnesium?
Not directly. Spironolactone is actually potassium and magnesium sparing by its primary mechanism of action. However, in some women it can trigger an indirect chain of events that leads to meaningful magnesium insufficiency. Spironolactone is more commonly associated with diarrhea than constipation — and when diarrhea is sustained, rapid intestinal transit time prevents adequate magnesium absorption, leading to progressive loss through the stool. Chronic gastrointestinal disturbance is one of the primary mechanisms of magnesium deficiency, and it doesn’t require dramatic symptoms to become clinically significant. The picture can become paradoxical: spironolactone triggers diarrhea, diarrhea impairs magnesium absorption, and magnesium insufficiency then disrupts gut motility — which is why some women on spironolactone eventually develop constipation as a downstream consequence. Sustained diarrhea also impairs absorption of zinc and vitamin A — two nutrients essential for acne prevention and control — as well as other fat-soluble vitamins. And when magnesium falls low enough to impair ATP synthesis, cellular energy production in the hair follicle becomes inefficient, creating the low-oxygen anaerobic environment in which Cutibacterium acnes thrives and produces the pro-inflammatory fatty acids that drive acne lesions. This is not a universal effect — not every woman on spironolactone will follow this path. But for those experiencing gastrointestinal symptoms while on the medication, testing with the Vibrant Wellness Micronutrient panel with SNPs is the most precise way to identify whether these depletions are present and how significant they are.
Is spironolactone safe to take long-term for acne?
Spironolactone is generally considered safe for most healthy women in the short to medium term. However, long-term use carries systemic considerations that are rarely discussed in a dermatology setting — including magnesium depletion, chronic skin dehydration from its diuretic action, potential adrenal and thyroid effects, and the ongoing suppression of symptoms without treatment of root causes. These are important factors to discuss with your prescribing provider, particularly if you are experiencing fatigue, mood changes, digestive symptoms, or other signs of systemic imbalance while on the medication.
What is the connection between insulin resistance and hormonal acne?
Insulin resistance is one of the most underrecognized drivers of hormonal acne in women. When blood sugar runs consistently high and insulin output spikes in response, the ovaries receive a signal to produce more androgens. Higher androgens increase sebum production, clog pores, and drive the inflammatory cascade that produces acne — particularly along the jawline, chin, and lower cheeks. This is also why hormonal acne and PCOS are so closely linked, as insulin resistance is central to both conditions. Addressing blood sugar dysregulation through diet, lifestyle, and targeted supplementation is often one of the first and most impactful steps in a functional medicine approach to clearing acne.
What skincare should I use while addressing hormonal acne from the inside out?
The most important principle when treating hormonal acne through a functional medicine approach is to treat the skin as sensitive first. This means avoiding harsh exfoliants, high-concentration actives, and stripping cleansers that compromise the skin barrier — particularly relevant for women on or coming off spironolactone, whose skin may already be affected by chronic dehydration. A gentle oil-based first cleanse, vitamin A-based moisturizers to normalize cell turnover and regulate oil production, targeted spot treatment for active lesions, and barrier-supportive reparative products form the foundation of an effective topical protocol alongside internal work.
What is spironolactone and how does it work for acne?
Spironolactone is a prescription medication originally developed to treat high blood pressure, heart failure, and fluid retention. It works for acne by blocking androgen receptors and reducing the activity of male hormones — particularly testosterone and DHT — that stimulate the skin’s oil glands to overproduce sebum. Less sebum means fewer clogged pores and fewer breakouts. It is prescribed off-label for hormonal acne in women, meaning it has not received FDA approval specifically for this use, though it has been used in dermatology for this purpose for decades. While it can be effective at managing acne symptoms, it works by suppressing the hormonal signal at the surface level — not by addressing why androgen activity is elevated in the first place.
What should I know before starting spironolactone for acne?
Before starting spironolactone for acne, there are several things worth understanding that are rarely discussed in a standard dermatology appointment. First, spironolactone manages acne by suppressing androgen activity — it does not investigate or treat the upstream reasons your androgens are elevated, which may include insulin resistance, chronic stress, poor hormone clearance, nutrient insufficiencies or other imbalances. Second, the drug requires ongoing use to maintain results — acne frequently returns when it is stopped, sometimes more severely than before. Third, spironolactone is a diuretic with systemic effects that can include gastrointestinal disturbance, indirect effects on magnesium and other nutrient levels, and — with long-term use — potential impact on adrenal and thyroid function. Fourth, if you are also experiencing fatigue, mood changes, bloating, irregular periods, brain fog, or sugar cravings alongside your acne, these symptoms are likely connected to the same root cause driving your breakouts — and spironolactone will not address them. Understanding the full picture before starting the medication gives you the best foundation for making an informed decision.
Will my acne get worse before it gets better on spironolactone?
Some women do experience an initial worsening of acne in the first few weeks of starting spironolactone, though this is not universal. What is commonly described as a purge — a temporary increase in breakouts as the drug begins to work — can happen as sebum production and hormonal activity shift. However, it is worth noting that not all worsening in the early weeks is a purge in the traditional sense. For some women, the gastrointestinal effects of spironolactone — particularly diarrhea — can begin to impair absorption of key skin nutrients like zinc and vitamin A early in treatment, which may independently contribute to skin reactivity before any hormonal benefit is established. If your acne is worsening significantly beyond the first six to eight weeks, or if you are experiencing systemic symptoms alongside it, that is worth investigating rather than waiting out.
Does spironolactone work for cystic acne?
Spironolactone can reduce cystic acne in women when the cysts are driven primarily by androgen excess and excess sebum production — which is often the case with deep, painful lesions along the jawline, chin, and lower cheeks that flare cyclically with the menstrual cycle. For this pattern, androgen suppression can produce meaningful improvement. However, cystic acne is also one of the strongest signals that something significant is happening systemically. Deep, inflammatory, cystic breakouts that are resistant to treatment — or that return after stopping spironolactone — often point to a more complex picture involving insulin resistance, gut dysbiosis, environmental toxin burden, impaired hormone metabolism, or a combination of these drivers. In these cases, suppressing androgen activity addresses the end result but leaves the underlying physiology intact. A functional medicine workup is particularly valuable for women with persistent cystic acne because it can identify exactly which internal drivers are fueling the most severe presentations.
What happens when I stop taking spironolactone for acne?
When spironolactone is stopped — particularly if stopped abruptly — acne frequently returns, and for many women it returns more severely than before. This rebound happens through two simultaneous mechanisms. First, the internal imbalances that were driving androgen excess before the medication — insulin resistance, adrenal dysregulation, poor hormone clearance, nutrient insufficiencies — have continued untreated throughout the time on the drug and resurface immediately when the androgen suppression is removed. Second, if spironolactone has contributed to gastrointestinal disturbance and downstream nutrient depletion during the time it was taken, the skin may now be more vulnerable than it was at the start — lower in the zinc, vitamin A, and magnesium it needs to regulate oil production, support immune function, and maintain healthy cell turnover. The most effective way to come off spironolactone is gradually and in parallel with a functional medicine program that is already addressing the root causes — so that when the drug is removed, the internal environment has shifted enough to support clearer skin without pharmaceutical suppression.
How does spironolactone compare to other acne treatments?
Spironolactone, oral antibiotics, the birth control pill, and isotretinoin (Accutane) are the most commonly prescribed systemic acne treatments in conventional dermatology. Each works through a different mechanism — spironolactone suppresses androgens, antibiotics target acne-associated bacteria, the pill regulates hormonal fluctuations, and isotretinoin dramatically reduces sebum production and normalizes skin cell turnover. All four share a fundamental limitation: they treat the downstream expression of acne without investigating or correcting the upstream drivers. Acne returns after stopping any of them when the root cause has not been addressed. From a functional medicine perspective, the more meaningful comparison is not between these medications but between a symptom-management approach and a root-cause approach — one that comprehensively reviews health history, symptoms and uses comprehensive testing to identify exactly what is driving the hormonal imbalance, metabolic dysfunction, or nutrient insufficiency behind the breakouts, and corrects those drivers directly. For women who have cycled through multiple acne medications without lasting results, this distinction is often the missing piece.
Written by Natalie Maibenko – a Certified Functional Medicine Practitioner and Master Esthetician with 22+ years of experience and founder of Unique Verve

With love and gratitude,
Natalie Maibenko
Functional Medicine & Skincare Expert – Helping You Take Control of Your Health and Achieve Lasting Skin Results
As a Certified Functional Medicine Practitioner my Expertise Encompasses:
- Immune System: frequent illness, UTIs, yeast infections
- Allergies, Asthma
- Skin Problems: acne, cystic acne, rosacea, eczema, dermatitis, ichthyosis, psoriasis, vitiligo, melasma
- Inflammation: arthritis, rhinitis, joint & muscle pain, migraines, headaches
- Sleep Disturbunces, Insomnia
- Gut Problems: IBS/IBD, bloating, acid reflux, gas, constipation, diarrhea, parasites, fungal/yeast overgrowths
- Hormonal Imbalances: PCOS, PMS symptoms, weight problems/inability to lose weight, thyroid problems
- Hair Loss, Alopecia
- Mood Imbalances: anxiety, depression, irritability
- Metabolic Dysfunction, Insulin Resistance, Type 2 Diabetes
- Optimizing Wellness for Successful Pregnancy
- Autoimmune Conditions: Hashimoto’s thyroiditis, grave’s disease, reumatoid arthritis (RA), lupus, etc
- Bone Health: osteopenia/ osteoporosis
- Effective Anti-Aging Strategies without Injectables with the inside-out & outside-in approach
- Detoxification of Heavy Metals, Mycotoxins, Environmental Toxins
- Reversing Breast Implant Illness
- Preparation for the Explant Surgery and Optimization of Wellness & Vitality Post-Explant
DISCLAIMER:
Information and content on this website is provided for educational purposes only, and is not intended to diagnose, treat and to be a substitute for the advice provided by your physician or other healthcare professional. No information offered here should be interpreted as a diagnosis of any disease, nor an attempt to treat or prevent or cure any disease or condition.
If you have any concerns or questions about your health, you should always consult with a physician or other healthcare professional. Do not disregard, avoid, or delay obtaining medical or health-related advice from your healthcare professional. Always speak with your healthcare professional before taking any medications, supplements or pursuing any wellness programs. Information provided on this website does not create a doctor-patient relationship between you and any professional affiliated with this website.