
Introduction to Histamine Rosacea Gut Connection
Histamine rosacea gut connection — three words that rarely appear together in a dermatology office, but that describe one of the most clinically significant and consistently overlooked drivers of rosacea I see in my functional medicine and functional dermatology practice.
You’ve tried azelaic acid, metronidazole, low-dose doxycycline. Maybe brimonidine for the persistent redness. The pimples calm down. The flushing comes back. The skin reacts to things it never used to. You’ve eliminated wine, spicy food, and anything remotely triggering — and still, the flares continue.
What most conventional rosacea treatment never investigates is the internal cascade that is producing the reactivity in the first place. In a significant subset of my rosacea patients, the central driver is a histamine-gut axis — a chain of interconnected dysfunction involving gut dysbiosis, impaired intestinal barrier integrity, DAO enzyme insufficiency, food sensitivities, thyroid dysfunction, nutrient depletion, and chronic immune activation — that keeps mast cells in a state of perpetual reactivity and the skin in a state of perpetual inflammation.
This post breaks down exactly how that cascade works, why it is so frequently missed, and what identifying and addressing it actually looks like clinically. As always, everything I cover here is informed by what I see in comprehensive functional medicine testing, and every protocol I build is individualized to what your specific results reveal.
What Conventional Rosacea Treatment Is Missing
The standard approach to rosacea — topical antibiotics, oral doxycycline, alpha-adrenergic agonists like brimonidine and oxymetazoline, and in severe cases immunosuppressants — manages the visible manifestations of inflammation without asking what is producing it. These treatments can provide meaningful short-term relief, but they share a fundamental limitation: they do not address the upstream drivers.
Oral antibiotics like doxycycline are particularly problematic in the long term. While they reduce inflammatory papules temporarily, chronic antibiotic use decimates the gut microbiome — the very ecosystem responsible for histamine breakdown, immune regulation, and gut barrier integrity. In patients whose rosacea is being driven by gut dysbiosis and histamine overload, long-term antibiotic use can paradoxically worsen the internal environment driving their flares, even as it quiets the skin surface temporarily.
Alpha-adrenergic agonists that constrict blood vessels address visible redness without touching the mast cell activation and histamine excess producing it. And when the medication wears off, the redness returns — often with a rebound effect.
The question that conventional treatment rarely asks is: why has this patient’s histamine threshold dropped so low that ordinary foods, environmental exposures, and hormonal fluctuations are producing an outsized inflammatory response? The answer, consistently, is upstream — in the gut, the thyroid, the nutrient status, and the immune system.
The Histamine Rosacea Gut Connection Cascade: How It All Connects
In functional medicine, we look at the body as an interconnected system. The histamine-rosacea connection is not a single mechanism — it is a cascade of interconnected dysfunctions that feed and amplify each other. Understanding how they connect is essential to understanding why addressing any single piece in isolation rarely produces lasting results.
1. Thyroid Dysfunction: The Overlooked Starting Point
Low thyroid function is one of the most frequently missed upstream drivers in histamine-driven rosacea — and one of the most impactful when identified. The connection is not immediately obvious, but clinically it is consistent and significant.
The thyroid governs metabolic rate across every organ system, including the digestive system. When thyroid function is suboptimal, digestive secretions decline — stomach acid production slows, bile output decreases, and digestive enzyme activity is reduced. These secretions are not just digestive aids. They are the gut’s primary defense against microbial overgrowth. Adequate stomach acid creates an inhospitable environment for pathogenic bacteria and parasites. Bile has direct antimicrobial properties. When these secretions are insufficient, the conditions for dysbiosis, SIBO, and even parasitic overgrowth are created.
In my functional medicine practice, I look at the full thyroid panel — TSH, free T3, free T4, reverse T3, and both thyroid antibodies (TPO and anti-thyroglobulin). Through a functional medicine lens, a TSH above 2 already suggests some degree of suboptimal thyroid function — a threshold that is significantly more conservative than the conventional range of up to 4.5. A patient who has been told her thyroid is “normal” based on TSH alone may have free T3 in the lower third of the reference range, elevated reverse T3 competing at receptor sites, or thyroid antibodies indicating early autoimmune activity — all of which impair thyroid function at the cellular level without triggering a conventional diagnosis.
The consequence for rosacea: sluggish thyroid → reduced digestive secretions → dysbiosis and malabsorption → nutrient insufficiencies → impaired DAO enzyme production and histamine breakdown → histamine accumulation → mast cell activation → rosacea flares. Addressing thyroid function is not a peripheral intervention in this clinical picture. It is often the upstream correction that makes everything else possible.
2. Gut Dysbiosis, Leaky Gut, and LPS Translocation
Whether initiated by thyroid dysfunction, antibiotic use, dietary patterns, chronic stress, or a combination, gut dysbiosis creates the intestinal environment in which histamine-driven rosacea thrives.
Dysbiosis — an imbalance in the gut microbiome characterized by reduced beneficial bacteria, increased pathogenic or opportunistic organisms, and reduced microbial diversity — impairs the gut’s capacity to regulate immune signaling, produce DAO enzyme, metabolize histamine-producing bacteria, and maintain the integrity of the intestinal lining.
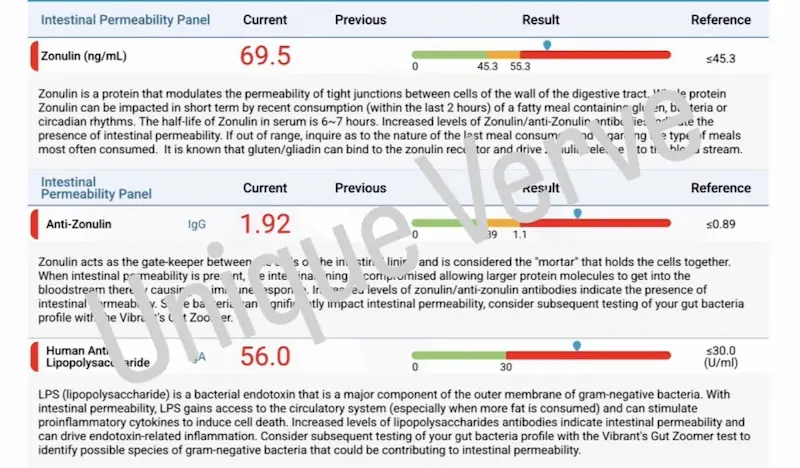
Leaky gut (enhanced intestinal permeability) is a direct consequence of dysbiosis and reduced microbial diversity. When tight junctions between intestinal epithelial cells are compromised, lipopolysaccharides (LPS) — fragments of gram-negative bacterial cell walls — translocate into the bloodstream. LPS is a potent activator of the innate immune system and a direct trigger of mast cell degranulation. Elevated anti-LPS antibodies on testing provide objective evidence that this translocation is occurring and that the immune system is actively responding to bacterial fragments in circulation — a pattern I see consistently in rosacea patients with significant gut involvement.
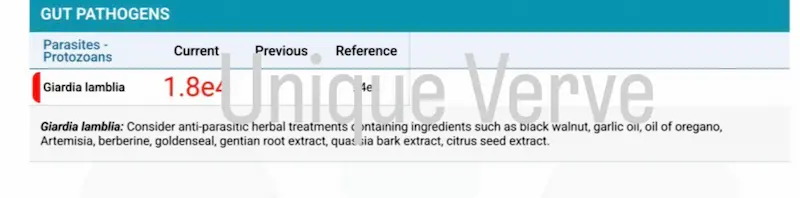
Parasitic infection adds another layer. Parasites activate mast cells directly through immune hypersensitivity responses, damage the intestinal lining, and create the conditions for secondary dysbiosis and nutrient malabsorption. In clinical practice, parasitic burden is far more common than most patients anticipate — and it is invisible without comprehensive stool testing.
3. DAO Enzyme Insufficiency and Histamine Accumulation
Diamine oxidase (DAO) is the primary enzyme responsible for breaking down histamine in the gut. When the intestinal lining is damaged — by dysbiosis, leaky gut, nutrient deficiencies, or chronic inflammation — DAO production is impaired, and histamine that would normally be degraded in the gut accumulates and enters systemic circulation.
DAO enzyme production requires specific nutrient cofactors — most critically vitamin B6, copper, and vitamin C. When these nutrients are depleted, DAO activity is further compromised regardless of how intact the gut lining is. This is why nutrient status is not a secondary consideration in histamine-driven rosacea — it is a primary clinical variable.
Vitamin B6 deserves specific attention. B6 is essential not only for DAO enzyme production but also for the methylation cycle — the biochemical pathway through which histamine is broken down systemically via the HNMT enzyme. Women who have taken oral birth control pills are at particular risk: OBC depletes the full spectrum of B vitamins, including B6, B9 (folate), and B12. A woman who took OBC for years in her 20s and 30s and develops rosacea in her late 30s or 40s may have a B vitamin depletion history that has never been identified or addressed — and that depletion may be directly impairing both her DAO enzyme production and her systemic histamine clearance.
Methylation is not just a histamine conversation — it is the same biochemical pathway responsible for safely clearing estrogen metabolites through Phase II liver detoxification. Impaired methylation from B vitamin depletion or MTHFR variants simultaneously reduces histamine breakdown and estrogen clearance, which is why the two conditions so frequently co-exist. The connection between poor estrogen clearance and inflammatory skin conditions is explored in depth here.
The MTHFR genetic variant compounds this further. MTHFR is one of the most common SNPs in the population and impairs the body’s ability to convert folate into its active form — reducing methylation capacity and consequently the ability to break down histamine systemically. In a woman with MTHFR who is also nutrient-depleted, exposed to environmental toxins, and dealing with gut dysbiosis, the histamine bucket fills faster than it can be cleared — and the skin becomes the most visible expression of that overflow.
4. Food Sensitivities: The Most Unacknowledged Source of Chronic Mast Cell Activation
Food sensitivities are categorically different from food allergies. They do not produce immediate IgE-mediated reactions. Instead, they create delayed, low-grade immune activation — a chronic, smoldering inflammatory response that operates beneath the threshold of obvious symptoms while continuously stimulating mast cells and sustaining systemic inflammation.
What makes food sensitivities particularly insidious in rosacea is that the foods driving immune activation are almost always foods the patient eats regularly — often foods she considers healthy and would never suspect. This is the clinical reality: the immune system develops reactivity to whatever it is chronically exposed to. Frequency of exposure, not inherent inflammatory potential, is the primary driver of food sensitivity development.
One of the most striking examples I see in practice is a patient whose comprehensive food sensitivity panel revealed reactivity to green tea, avocado, olive, and parsley — among others. These are foods that appear on every anti-inflammatory diet recommendation. She had been eating them consistently, believing they were supporting her health. Instead, they had become antigens — sources of chronic immune activation that were sustaining her mast cell reactivity and driving her rosacea flares silently, continuously, and invisibly.
This is precisely why I often recommend comprehensive food sensitivity (available for my functional medicine clients) testing in my rosacea workup — and why elimination diets based on generic high-histamine food lists frequently fail. The foods driving immune activation in your body are specific to your immune system’s history of exposure. They cannot be identified by a list. They require testing.
5. Nutrient Insufficiencies and SNPs: The Missing Cofactors
The body’s capacity to manage histamine — both in the gut and systemically — depends on a specific set of nutrients functioning as enzymatic cofactors. When these nutrients are insufficient, histamine breakdown slows regardless of how well other aspects of the protocol are working.
Beyond vitamin B6 and the methylation B vitamins, vitamin A deserves specific attention in the histamine-gut-rosacea picture. Vitamin A is essential for the integrity of epithelial cells throughout the body — including both the gut lining and the skin. It plays a central role in immune regulation, including the modulation of mast cell activity and the defense against parasitic infection. Genetic variants (SNPs) affecting vitamin A metabolism — including variants in the BCMO1 gene that impairs conversion of beta-carotene to retinol — can result in functional vitamin A insufficiency even in patients eating a diet rich in vitamin A precursors.
In practice, I assess nutrient status and SNPs together through the micronutrient panel with genetic variants. The clinical picture they reveal is often the missing piece that explains why a patient has not responded to previous interventions — her body lacks the biochemical infrastructure to execute the histamine breakdown pathways, regardless of what else is being addressed.
Vitamin D is equally important. Vitamin D insufficiency is associated with gut dysbiosis, impaired tight junction integrity, and dysregulated immune function — all of which amplify the histamine-rosacea cascade. And vitamin D deficiency is extraordinarily common, particularly in women who avoid sun exposure as a rosacea trigger and use SPF regularly — creating a clinical irony where the very behavior intended to manage rosacea worsens an underlying driver.
A Patient Story: When the Healthiest Foods Are the Problem
One of my patients came to me with persistent rosacea — flushing, chronic redness, and a pattern of reactivity that seemed to have no consistent trigger. She had tried multiple conventional treatments with partial results but no lasting clearance. She also had significant digestive symptoms — bloating, irregular bowel habits, and what she described as a generally reactive gut — alongside seasonal allergies, frequent illness, and significant mood imbalances including anxiety, irritability, and depression that she had been managing separately.
She was eating what she considered an exemplary anti-inflammatory diet. Green tea every morning. Avocado daily. Generous use of olive oil and fresh herbs including parsley. She had eliminated alcohol, processed foods, and anything on the standard rosacea trigger list. Her skin continued to flare.
Comprehensive testing told a different story. Her food sensitivity panel revealed significant immune reactivity to green tea, avocado, olive, and parsley — alongside several other foods she consumed regularly. The foods she had built her anti-inflammatory diet around had become the primary antigens driving her chronic immune activation.
Her Gut Zoomer revealed high levels of parasitic infection alongside significant dysbiosis — a combination that was directly driving mast cell activation, gut lining damage, and systemic immune dysregulation. Her Wheat Zoomer showed markedly elevated intestinal permeability markers and high anti-LPS antibodies — objective evidence of active LPS translocation into circulation and a systemic immune response to bacterial fragments. Her micronutrient panel with SNPs revealed genetic variants affecting B vitamin metabolism and vitamin A conversion, alongside low cellular levels of both — explaining both her impaired DAO enzyme production and her compromised immune defense against the parasitic burden.
The mood imbalances — anxiety, irritability, depression — were not a separate clinical problem. They were downstream of the same gut-driven systemic inflammation and nutrient insufficiency producing her rosacea. Histamine excess directly affects neurotransmitter balance. LPS translocation drives neuroinflammation. B vitamin depletion impairs serotonin and dopamine synthesis. The gut and the brain were expressing the same upstream dysfunction through different channels.
Her protocol addressed the full picture systematically: parasite clearance, gut restoration, targeted nutrient repletion including methylated B vitamins and vitamin A, food antigen removal, and progressive barrier restoration topically. Her rosacea improved significantly. Her digestion normalized. Her mood stabilized. None of these outcomes were separate — they were all downstream of the same upstream imbalances being corrected.
Testing: What I Look For and Why
While every workup is tailored to the individual, the following panels give me the most clinically meaningful picture in histamine-gut rosacea cases — and here is why each one matters.
Full Thyroid Panel
TSH, free T3, free T4, reverse T3, TPO antibodies, and anti-thyroglobulin antibodies. I am looking at the complete picture of thyroid function — not just TSH. Through a functional medicine lens, a TSH above 2 warrants investigation of the full panel in context. Suboptimal thyroid function impairing digestive secretions is frequently the most upstream correctable driver in the histamine-gut-rosacea cascade and is missed by conventional testing that relies on TSH alone.
Comprehensive Food Sensitivity Panel
IgG and IgA-mediated food sensitivity testing across a broad panel of foods. Because reactivity develops to foods consumed regularly — not to inherently inflammatory foods — a comprehensive panel is essential. Generic high-histamine elimination diets miss the specific antigens driving immune activation in each individual patient. This is one of the highest-impact tests in the rosacea workup.
Gut Zoomer
Comprehensive stool analysis assessing microbiome composition, pathogenic organisms including parasites, inflammatory markers, digestive markers. The Gut Zoomer provides the most complete picture of the microbial and structural gut environment available through functional medicine testing.
Wheat Zoomer
Assessment of intestinal permeability, anti-LPS antibodies, wheat sensitivity markers, and gluten-related immune reactivity. Elevated anti-LPS antibodies provide objective evidence of LPS translocation into circulation — direct confirmation that leaky gut is driving systemic immune activation. This is a critical data point in histamine-driven rosacea cases with significant gut involvement.
Micronutrient Panel with SNPs
Cellular levels of vitamins, minerals, amino acids, and antioxidants alongside genetic variants affecting nutrient metabolism. B vitamins (B6, B9, B12), vitamin A, vitamin D, copper, and zinc are the most clinically relevant nutrients in the histamine-gut-rosacea picture. SNPs affecting methylation (MTHFR), vitamin A conversion (BCMO1), and B vitamin metabolism directly inform the protocol and explain why standard supplementation may be insufficient without addressing the genetic variants affecting absorption and utilization.
Total Tox Burden
Heavy metals, mycotoxins, and environmental chemicals. Toxic burden increases nutrient demand, impairs liver detoxification of histamine and estrogen, and directly activates mast cells. In patients with MTHFR variants, toxic exposure has an amplified impact because impaired methylation reduces the body’s detoxification capacity simultaneously.
Standard Metabolic Markers
Fasting insulin, HbA1C, CMP, and lipid panel. Blood sugar dysregulation, liver enzyme elevation, and metabolic markers provide important context for the full inflammatory picture and help identify additional upstream drivers.
The Functional Medicine Approach: Internal and Topical
While every protocol is individualized to what health history and testing reveals, the following represents the clinical framework I work within for histamine-gut rosacea cases. The internal protocol targets the full cascade — thyroid support, gut restoration, histamine breakdown, nutrient repletion, and immune regulation. The topical approach is deliberately conservative, prioritizing barrier protection over active intervention.
Internal Support
- GI MaxAid — gut lining repair and restoration of intestinal barrier integrity, directly supporting DAO enzyme production in the epithelial lining and reducing LPS translocation.
- Methylated B-Complex — methylated forms of B6, B9, and B12 to support DAO enzyme production, systemic histamine breakdown through the HNMT pathway, and methylation capacity — essential for patients with MTHFR variants and those with OBC-related B vitamin depletion history.
- Probiotic Integrum — a clinically selected probiotic formulation chosen specifically for its histamine-conscious strain profile. Not all probiotics are appropriate in histamine-driven rosacea — certain strains produce histamine and can worsen the picture. Strain selection matters significantly in this clinical context.
- BioC with Bioflavonoids — vitamin C as a DAO cofactor and natural antihistamine, reducing mast cell histamine release and supporting vascular integrity.
- Omega3 BioPure — systemic anti-inflammatory foundation, mast cell membrane stabilization, and skin barrier lipid support.
- EssentialA / Vitamin A support — for patients with vitamin A SNPs or low cellular levels, targeted vitamin A repletion supports gut epithelial integrity, balanced immune function including defense against parasitic infection, and skin barrier health. Dosing and form are individualized based on testing.
Topical Support: Conservative Barrier First
Histamine-driven rosacea with an impaired barrier requires the most conservative topical approach of any rosacea presentation. The skin is already in a state of heightened reactivity — introducing too many actives too soon will worsen sensitization rather than improve it. The clinical priority is barrier protection and stabilization before any active intervention.
For most patients in the acute or highly reactive phase, I begin with only:
- Environ Pre-Cleansing Oil — gentle lipid-based cleansing that removes impurities without stripping the acid mantle or compromising barrier integrity.
- Environ ACE Body Oil — rich in vitamins A, C, and E in a nourishing lipid base that supports barrier repair and provides antioxidant protection without triggering reactivity.
- Broad-spectrum SPF (Tizo or Environ RAD) — non-negotiable. UV exposure is a direct mast cell activator. SPF is the single most important topical intervention in any rosacea presentation and the one that must be maintained consistently regardless of what else is being used.
This is deliberately minimal. The internal protocol is doing the primary work — reducing mast cell activation, restoring gut integrity, clearing histamine load, and repairing the internal drivers of barrier compromise. As internal inflammation resolves and the skin stabilizes, additional topical support including vitamin A introduction can be considered gradually. All topical recommendations are individualized.
The Most Important Thing to Understand About Histamine-Driven Rosacea
If there is one insight I want every woman with persistent rosacea to carry from this post, it is this: the histamine bucket doesn’t overflow because of one thing. It overflows because of the accumulation of unaddressed upstream drivers — suboptimal thyroid function creating the conditions for gut dysbiosis, maldigestion and malabsorption leading to nutrient insufficiencies, genetic variants reducing the body’s capacity to break down histamine, food sensitivities creating a continuous and unacknowledged source of mast cell activation, parasitic or pathogenic burden sustaining immune dysregulation — all compounding silently until the threshold is crossed and the skin can no longer contain the internal inflammatory load.
Identifying which specific combination of drivers is active in your body is the only way to build a protocol that actually works. That requires thorough investigation of your health history, symptoms and testing (although not always necessary). It requires going upstream. And it requires a clinical framework that sees the gut health, the thyroid, the immune system, and the skin as the interconnected system they are.
This is the foundation of my functional medicine and functional dermatology practice. The skin is the signal. The work is internal.
The functional medicine approach to rosacea does not rely on antibiotics or prescriptions. It relies on identifying what is specifically driving your histamine overload — and addressing that systematically.
I offer virtual Initial Functional Medicine Health and Skin Assessments for anyone who are ready to look upstream. This is where we take a full picture of your health history, your current symptoms, and the patterns that connect them — and build a testing and protocol strategy specific to your body.
→ Book your Initial Functional Medicine Health and Skin Assessment
Frequently Asked Questions
What is the connection between histamine and rosacea?
Histamine is released by mast cells in the skin in response to immune triggers, causing vascular dilation, flushing, and redness. In histamine-driven rosacea, mast cells are chronically activated by internal drivers — gut dysbiosis, leaky gut, food sensitivities, nutrient deficiencies, and thyroid dysfunction — producing a persistent state of histamine excess that the body cannot break down fast enough. The result is the chronic vascular reactivity and inflammation characteristic of rosacea. Addressing the upstream drivers of mast cell activation — not just suppressing the histamine response — is what produces lasting improvement.
Can gut health affect rosacea?
Yes — significantly. The gut drives rosacea through multiple interconnected mechanisms: dysbiosis impairs DAO enzyme production needed to break down histamine; leaky gut allows bacterial fragments (LPS) into circulation, activating mast cells systemically; parasitic infection triggers immune hypersensitivity and gut lining damage; and a disrupted microbiome impairs the immune regulation needed to keep inflammatory signaling calibrated. In many rosacea patients, restoring gut integrity is the single highest-impact intervention in the entire protocol.
Can histamine in food cause rosacea?
Partially — but the more important and more overlooked answer is that it is not just high-histamine foods that drive rosacea. Food sensitivities develop to foods consumed regularly, regardless of their histamine content. The immune system creates reactivity to whatever it is chronically exposed to — which means the avocado, green tea, or olive oil you eat every day can become a more significant source of mast cell activation than a glass of wine you drink occasionally. Generic high-histamine elimination diets miss this entirely. Comprehensive food sensitivity testing identifies the specific antigens driving immune activation in your body — which is the only way to know which foods are actually contributing to your rosacea.
How does thyroid function affect rosacea and histamine?
Low thyroid function reduces the production of stomach acid, bile, and digestive enzymes — the gut’s primary defenses against microbial overgrowth. When these secretions are insufficient, dysbiosis develops, creating the conditions for leaky gut, impaired DAO enzyme production, nutrient malabsorption, and histamine accumulation. Through a functional medicine lens, a TSH above 2 warrants full thyroid panel investigation — including free T3, reverse T3, and both antibodies — because suboptimal thyroid function that falls within conventional normal ranges can be a significant upstream driver of the entire histamine-gut-rosacea cascade.
Can birth control pills cause rosacea or histamine intolerance?
Oral birth control pills deplete the full spectrum of B vitamins — including B6, B9, and B12 — which are essential cofactors for DAO enzyme production in the gut and systemic histamine breakdown through the methylation pathway. A woman who took oral birth control for years and develops rosacea or histamine intolerance in her late 30s or 40s may have a B vitamin depletion history that has never been identified or corrected. Combined with MTHFR genetic variants — which are extremely common and further impair B vitamin metabolism and methylation — this depletion can significantly reduce the body’s capacity to manage histamine over time.
Why does my rosacea flare even when I eat healthy?
Because the foods driving your immune activation may be the ones you consider healthiest. Food sensitivities develop through chronic exposure, not through the inherent inflammatory potential of a food. Green tea, avocado, olive oil, and fresh herbs are examples of foods I have seen drive significant rosacea flares through immune reactivity in patients who had built their entire diet around them. Without comprehensive food sensitivity testing, these antigens remain invisible — a continuous, unacknowledged source of mast cell activation that no amount of trigger avoidance or topical treatment can address.
Why does my rosacea get worse after eating?
Post-meal rosacea flares are one of the most consistent signs that food sensitivities or histamine dysregulation are driving your skin. When you eat a food your immune system has developed reactivity to, the resulting immune activation triggers mast cell degranulation and histamine release — producing flushing, redness, and increased reactivity within hours of eating. Because food sensitivity reactions are delayed 24–72 hours rather than immediate, the connection between a specific food and a skin flare is almost never obvious without systematic testing. If your rosacea consistently worsens after meals, comprehensive food sensitivity testing is the most clinically meaningful next step.
Is my rosacea actually a food intolerance?
It may be a significant part of the picture — but food intolerance is rarely the sole driver. In functional medicine, food sensitivities are one of the most consistently underidentified contributors to rosacea because the reactions are delayed, the foods involved are often considered healthy, and no conventional rosacea workup includes food sensitivity testing. What I see clinically is that food sensitivities operate as a continuous, unacknowledged source of chronic immune activation and mast cell stimulation — compounding other internal drivers like gut dysbiosis, thyroid dysfunction, and nutrient insufficiency. Identifying and removing food antigens is frequently one of the highest-impact initial interventions, but it works best as part of a comprehensive root-cause protocol rather than in isolation.
Does eliminating foods really help rosacea?
It depends entirely on which foods you eliminate and how you identify them. Generic elimination diets based on high-histamine food lists help some patients partially — but they miss the individual-specific antigens that comprehensive testing reveals. A patient who eliminates wine and spicy food but continues eating green tea, avocado, and olive oil daily — all of which are showing as significant immune antigens on her food sensitivity panel — will see limited improvement. Elimination works when it is guided by actual testing rather than by lists. And for most patients, food antigen removal needs to be accompanied by gut restoration and nutrient repletion to produce lasting results — because the underlying dysbiosis and DAO insufficiency that allowed histamine to accumulate in the first place must also be addressed.
Why doesn’t my dermatologist mention histamine?
Because histamine-driven rosacea requires an internal investigation that falls outside the dermatology scope of practice. Dermatology is trained to diagnose and manage skin conditions — not to assess gut microbiome composition, thyroid function, food sensitivity panels, or methylation genetics. The histamine-mast cell-rosacea connection is well-established in the research, but it requires functional medicine testing and a systems-based clinical framework to identify and address. This is not a criticism of dermatologists — it is a structural limitation of a specialty that focuses on the organ rather than the upstream drivers producing the condition. The functional medicine and functional dermatology approach exists specifically to fill this gap.
Why is my rosacea resistant to medication?
Medication-resistant rosacea is almost always a sign that the upstream internal drivers have not been identified or addressed. Antibiotics, topical prescriptions, and vascular-constricting agents manage the visible manifestations of inflammation without touching the mast cell activation, histamine overload, gut dysbiosis, food sensitivities, thyroid dysfunction, or nutrient insufficiency producing it. When the medication wears off — or when the gut microbiome is sufficiently disrupted by long-term antibiotic use — the internal inflammatory environment reasserts itself and the flares return. Medication resistance is not a skin problem. It is a signal that the investigation needs to go upstream.
Why do I get hives alongside my rosacea?
Hives and rosacea appearing together is a strong clinical signal of significant mast cell activation and histamine excess. Both conditions share the same underlying mechanism — mast cells degranulating and releasing histamine into skin tissue — which is why they co-occur in patients with a high total histamine burden. When the histamine bucket is full enough to produce hives, it is almost certainly full enough to be driving the vascular reactivity and flushing of rosacea simultaneously. The presence of both conditions together typically indicates that the upstream drivers — gut dysbiosis, food sensitivities, nutrient insufficiency, toxic burden, or hormonal imbalance — are creating a particularly high mast cell activation load that warrants comprehensive investigation rather than symptomatic management of each condition separately.
Why haven’t multiple diets helped my rosacea?
Because the foods driving your immune activation are specific to your immune system — and no generic diet can identify them. Anti-inflammatory diets, low-histamine diets, elimination diets, and gut-healing protocols all operate on population-level assumptions about which foods are inflammatory. But food sensitivity reactivity is individual. Your immune system may be completely tolerant of foods on every “avoid” list while being significantly reactive to foods on every “eat more of” list. Until comprehensive food sensitivity testing identifies your specific antigens, dietary changes will produce inconsistent and incomplete results. Diet is a powerful tool in rosacea management — but only when it is guided by your individual testing data rather than by generalized protocols.
Can stress and histamine trigger rosacea together?
Yes — and they amplify each other through a direct physiological mechanism. Stress activates the HPA axis, elevating cortisol. Cortisol directly stimulates mast cells, increasing their sensitivity and lowering the threshold at which they degranulate in response to other triggers — including histamine-releasing foods, environmental exposures, and hormonal fluctuations. At the same time, chronic stress impairs gut barrier integrity, worsens dysbiosis, and reduces DAO enzyme activity — amplifying histamine accumulation from the gut side simultaneously. The result is a forward-feeding cycle: stress primes mast cells, histamine accumulates faster than it can be cleared, the skin becomes more reactive, visible worsening creates psychological distress, and cortisol rises further. Addressing the HPA axis and stress physiology is not a soft add-on to the rosacea protocol — it is a hard clinical driver that directly affects histamine load and mast cell reactivity.
Written by Natalie Maibenko – a Certified Functional Medicine Practitioner and Master Esthetician with 22+ years of experience and founder of Unique Verve

As a Certified Functional Medicine Practitioner my Expertise Encompasses:
- Immune System: frequent illness, UTIs, yeast infections
- Allergies, Asthma
- Skin Problems: acne, cystic acne, rosacea, eczema, dermatitis, ichthyosis, psoriasis, vitiligo, melasma
- Inflammation: arthritis, rhinitis, joint & muscle pain, migraines, headaches
- Sleep Disturbunces, Insomnia
- Gut Problems: IBS/IBD, bloating, acid reflux, gas, constipation, diarrhea, parasites, fungal/yeast overgrowths
- Hormonal Imbalances: PCOS, PMS symptoms, weight problems/inability to lose weight, thyroid problems
- Hair Loss, Alopecia
- Mood Imbalances: anxiety, depression, irritability
- Metabolic Dysfunction, Insulin Resistance, Type 2 Diabetes
- Optimizing Wellness for Successful Pregnancy
- Autoimmune Conditions: Hashimoto’s thyroiditis, grave’s disease, reumatoid arthritis (RA), lupus, etc
- Bone Health: osteopenia/ osteoporosis
- Effective Anti-Aging Strategies without Injectables with the inside-out & outside-in approach
- Detoxification of Heavy Metals, Mycotoxins, Environmental Toxins
- Reversing Breast Implant Illness
- Preparation for the Explant Surgery and Optimization of Wellness & Vitality Post-Explant
With love and gratitude,
Natalie Maibenko
Functional Medicine & Skincare Expert – Helping You Take Control of Your Health and Achieve Lasting Skin Results Nationwide — Virtual Practice
Disclaimer: Information and content on this website is provided for educational purposes only, and is not intended to diagnose, treat and to be a substitute for the advice provided by your physician or other healthcare professional. No information offered here should be interpreted as a diagnosis of any disease, nor an attempt to treat or prevent or cure any disease or condition. If you have any concerns or questions about your health, you should always consult with a physician or other healthcare professional. Do not disregard, avoid, or delay obtaining medical or health-related advice from your healthcare professional. Always speak with your healthcare professional before taking any medications, supplements or pursuing any wellness programs. Information provided on this website does not create a doctor-patient relationship between you and any professional affiliated with this website.