Introduction
Poor estrogen clearance rosacea connection — a phrase that captures one of the most clinically significant and most consistently missed drivers of inflammatory skin conditions in women, and one that standard hormone blood work is structurally incapable of revealing.
You may have had your hormones tested. You may have been told your estrogen levels are normal. And you may still be dealing with rosacea, hormonal acne, eczema, bloating, irritability, anxiety, depression, terrible PMS, sugar cravings, hair loss, and exhaustion — symptoms that collectively paint a clear picture of estrogen dominance, even when the numbers on a standard blood panel say otherwise.
This is not a contradiction. It is a gap in what conventional testing measures. Standard hormone blood work shows how much estrogen your body is producing. It does not show what your body is doing with that estrogen once it is produced — how it is being metabolized through the liver, which metabolic pathways it is preferring, what byproducts it is generating, and whether those byproducts are being safely cleared or accumulating in tissue. That information requires a different kind of testing entirely.
In my functional medicine and functional dermatology practice, the Vibrant Wellness Hormone Zoomer is the tool that reveals this picture. And what it shows — consistently, across a wide range of patients who present with inflammatory skin conditions and estrogen dominant symptoms alongside normal standard blood work — is that poor estrogen clearance is operating silently, producing metabolites that drive mast cell activation, systemic inflammation, and skin reactivity from the inside out.
This post explains exactly how estrogen metabolism works, what goes wrong when clearance is impaired, what it looks like on a lab result, and why understanding your estrogen metabolite pattern may be one of the most important things you can do for both your skin and your long-term hormonal health. As always, every protocol I build is individualized to what your specific testing reveals — what follows is the clinical framework I work within.
How Estrogen Is Actually Metabolized — And Why It Matters
Most discussions of estrogen focus on production — how much estrogen the body makes, whether levels are high or low, whether they are in range. What is almost never discussed is what happens to estrogen after it is produced. This is where the clinically significant story lives.
Estrogen metabolism occurs primarily in the liver through a two-phase detoxification process. Understanding these two phases — and what determines which metabolic pathways estrogen takes through them — is essential to understanding why two women with identical circulating estrogen levels can have completely different hormonal health outcomes.
Phase I: The Three Metabolic Pathways
In Phase I liver detoxification, estrogen is converted into one of three primary metabolites through hydroxylation. The pathway taken determines the downstream hormonal and inflammatory consequences:
2-Hydroxyestrone (2-OH-E1) — The Protective Pathway
The 2-OH pathway produces estrogen metabolites with weak estrogenic activity. These metabolites do not strongly activate estrogen receptors, do not significantly stimulate cell proliferation, and are associated with protective effects in hormone-sensitive tissues. Pushing estrogen metabolism toward the 2-OH pathway is the clinical goal. Cruciferous vegetables — broccoli, cauliflower, Brussels sprouts, kale — contain indole-3-carbinol and its gut-derived metabolite DIM, which specifically support 2-OH metabolism and are among the most clinically meaningful dietary interventions for estrogen clearance support.
16-Alpha-Hydroxyestrone (16-OH-E1) — The Estrogenic Pathway
The 16-OH pathway produces strongly estrogenic metabolites that bind actively to estrogen receptors and promote cell proliferation in hormone-sensitive tissues. When estrogen metabolism preferentially takes the 16-OH route, the result is a clinically estrogenic environment even when circulating estrogen levels appear within the normal reference range. This is the patient who has all the symptoms of estrogen dominance — bloating, constipation, terrible PMS, irritability, anxiety, depression, sugar cravings, acne, low energy, inflammatory skin flares — but whose standard blood work shows estrogen levels that are technically normal. The problem is not how much estrogen she is producing. It is where that estrogen is going metabolically.
4-Hydroxyestrone (4-OH-E1) — The DNA-Damaging Pathway
The 4-OH pathway is the most clinically serious of the three. The 4-OH metabolites are catechol estrogens that can form DNA adducts — directly binding to DNA and causing damage that, if not repaired, increases the risk of mutations in hormone-sensitive tissues. Research has specifically implicated elevated 4-OH-E1 in the initiation of sex hormone-sensitive cancers, including breast cancer. This is the metabolite pattern that makes estrogen clearance not just a symptom management conversation but a genuine cancer risk reduction conversation — one that extends far beyond BRCA genetics into epigenetics, nutrient status, liver function, and metabolic health. Many women believe that cancer risk related to hormones is determined primarily by BRCA gene status. This is a significant misconception. BRCA variants are one piece of a much larger picture. Poor estrogen clearance through the 4-OH pathway is an independently modifiable risk factor — and it is one that comprehensive hormone testing can identify and that targeted intervention can correct.
Phase II: Methylation and Clearance
Once Phase I metabolism has produced estrogen metabolites, Phase II detoxification is responsible for neutralizing and clearing them from the body — primarily through methylation, but also through sulfation and glucuronidation. Phase II is where the metabolites produced in Phase I are rendered water-soluble and prepared for excretion through bile and urine.
Methylation deserves particular attention because it is the most clinically relevant Phase II pathway in the context of estrogen clearance — and the one most commonly impaired. Methylation is a biochemical process involving the transfer of a methyl group that occurs in thousands of reactions throughout the body, including neurotransmitter synthesis, immune regulation, DNA repair, and detoxification. For estrogen clearance specifically, methylation converts the reactive 4-OH catechol estrogens into stable, excretable methoxy estrogens — effectively neutralizing their DNA-damaging potential.
When methylation is impaired — by nutrient deficiencies (B vitamins, magnesium, amino acids), COMT or MTHFR genetic variants, chronic stress, alcohol, or toxic burden — the 4-OH metabolites that should be safely methylated and cleared instead accumulate, increasing their opportunity to form DNA adducts and sustain systemic inflammation.
This is why methylation is not just an estrogen conversation. It is a master regulatory pathway whose function determines outcomes across virtually every system in the body — and why supporting methylation through targeted nutrient repletion and lifestyle factors is one of the highest-impact interventions in functional medicine.
What Drives Estrogen Down the Wrong Pathways
While every clinical picture is individual, the following factors consistently impair estrogen metabolism and push clearance toward unfavorable 16-OH and 4-OH pathways. Understanding these drivers is both clinically important and practically empowering — because most of them are modifiable.
Nutrient Insufficiencies and Methylation Cofactor Depletion
Methylation requires a specific set of nutrient cofactors — B vitamins (particularly B2, B6, B9, and B12), magnesium, and amino acids including methionine and glycine. When these nutrients are insufficient, methylation slows, Phase II clearance is impaired, and reactive estrogen metabolites accumulate. Women who have taken oral birth control pills are particularly vulnerable — OBC depletes the full B vitamin spectrum, directly impairing the methylation capacity needed for estrogen clearance. This depletion, if not corrected, can persist for years after discontinuing OBC.
COMT and MTHFR Genetic Variants
The COMT (catechol-O-methyltransferase) enzyme is directly responsible for methylating catechol estrogens — including the 4-OH metabolites — in Phase II. COMT variants reduce this enzyme’s activity, impairing the methylation of 4-OH-E1 and allowing it to accumulate. MTHFR variants reduce the conversion of folate to its active form, impairing the broader methylation cycle that COMT depends on. These variants are common in the general population (I personally carry both of these SNPs) and are identifiable through genetic SNP testing — making them actionable clinical information rather than fixed risks.
Gut Dysbiosis and Beta-Glucuronidase Activity
The gut and gut health plays a critical role in estrogen clearance through the estrobolome — the subset of gut bacteria that metabolize estrogen in the digestive tract. When gut dysbiosis is present, certain bacteria produce elevated beta-glucuronidase — an enzyme that deconjugates estrogen that has already been processed by the liver and prepared for excretion, allowing it to be reabsorbed into circulation. This effectively undoes the liver’s clearance work, recirculating estrogen and amplifying the estrogenic load regardless of how well the liver is functioning.
Constipation compounds this significantly. When transit time is slow, deconjugated estrogen has extended contact time with the intestinal wall and more opportunity for reabsorption. Addressing constipation is therefore not a peripheral intervention in estrogen clearance — it is a prerequisite. I always address gut health and bowel regularity before introducing liver support, because a congested gut will continue to reabsorb estrogen regardless of what the liver is doing.
Alcohol
Alcohol impairs both Phase I and Phase II liver detoxification, depletes B vitamins and magnesium, and increases estrogen levels by impairing its clearance. Even moderate alcohol consumption has measurable effects on estrogen metabolism — shifting it toward less favorable pathways and reducing methylation capacity simultaneously.
Toxic Burden and Xenoestrogens
Environmental toxins — particularly xenoestrogens found in conventional produce (glyphosate is a documented endocrine disruptor), conventional dairy, plastics, personal care products, and household chemicals — bind to estrogen receptors and mimic estrogenic activity in the body. They also compete for the same liver detoxification pathways as endogenous estrogen, increasing the overall burden on Phase I and Phase II and impairing clearance capacity. This xenoestrogenic burden is particularly significant in perimenopausal women, whose declining progesterone and shifting estrogen metabolism already create a more estrogenic internal environment — a connection explored in depth in our post on rosacea and perimenopause. A woman eating an otherwise clean diet but consuming conventional dairy and non-organic produce daily may be carrying a significant xenoestrogenic burden that her standard hormone testing will never reveal — but that a Total Tox Burden panel will.
Insulin Resistance, High Blood Sugar, and Chronic Stress
Insulin resistance and chronically elevated blood sugar impair liver detoxification function and promote inflammation that disrupts Phase I enzyme activity. Chronic stress elevates cortisol, which competes for detoxification resources, depletes methylation cofactors, and impairs gut integrity — amplifying every driver of poor estrogen clearance simultaneously. These are not peripheral lifestyle factors. They are direct biochemical impairments of the metabolic pathways responsible for clearing estrogen safely.
Dietary Factors
Conventional dairy and refined carbohydrates promote insulin resistance, gut dysbiosis, and inflammation — all of which impair estrogen clearance. Conventional produce carrying glyphosate residues adds xenoestrogenic burden. A diet low in cruciferous vegetables removes one of the most clinically meaningful dietary supports for 2-OH metabolism. Dietary intervention in estrogen clearance is not about a generic clean eating protocol — it is about specifically reducing xenoestrogenic burden and providing the nutrients and plant compounds that support favorable metabolic pathways.
Poor Estrogen Clearance Rosacea Connection: Why Your Skin Keeps Flaring
The connection between poor estrogen clearance and inflammatory skin conditions operates through three primary mechanisms — all of which converge on the same outcome: a chronically activated mast cell population producing persistent skin inflammation.
Mast Cell Stimulation Through Estrogen Dominance
Both the 16-OH and 4-OH metabolite patterns create a state of functional estrogen dominance — either through direct estrogenic receptor activation (16-OH) or through the systemic inflammation produced by accumulating reactive metabolites (4-OH). Estrogen directly stimulates mast cells, increasing their sensitivity and triggering histamine release which over time can lead to histamine intolerance. The result is the vascular reactivity, flushing, and redness characteristic of rosacea — driven not by how much estrogen is circulating, but by what form that estrogen has taken metabolically and how it is affecting mast cell behavior at the tissue level.
Systemic Inflammation From Reactive Metabolites
The 4-OH catechol estrogens are pro-inflammatory independently of their estrogenic effects. Their accumulation — when methylation is insufficient to clear them — sustains a state of systemic oxidative stress and inflammation that manifests in multiple ways simultaneously: on the skin as rosacea, eczema, hormonal acne, dermatitis, or psoriasis; in the gut as bloating, constipation, and dysbiosis; in the nervous system as anxiety, irritability, and depression; and in the immune system as allergies, frequent illness, and heightened reactivity.
Impaired Liver Detoxification Amplifying Every Other Driver
When liver detoxification is burdened by poor estrogen clearance, its capacity to clear histamine, toxins, and other inflammatory mediators is simultaneously reduced. The liver does not detoxify estrogen in isolation — it is processing a continuous load of compounds requiring clearance. When poor estrogen metabolism consumes detoxification resources, the burden on every other clearance pathway increases, amplifying the total inflammatory load that ultimately expresses itself on the skin.
The skin conditions I most consistently see in patients with poor estrogen clearance include rosacea, hormonal acne, eczema, contact dermatitis, and melasma. Psoriasis also has a significant connection — partly through impaired bile function affecting immune regulation in the skin. Each condition reflects the same upstream metabolic dysfunction expressing itself through a different skin phenotype.
Two Patient Stories: The Same Root Cause, Two Different Lab Patterns
One of the most clinically instructive aspects of poor estrogen clearance is that it presents differently on testing depending on which pathway is impaired — and both patterns can be symptomatic while being missed entirely by standard hormone blood work.
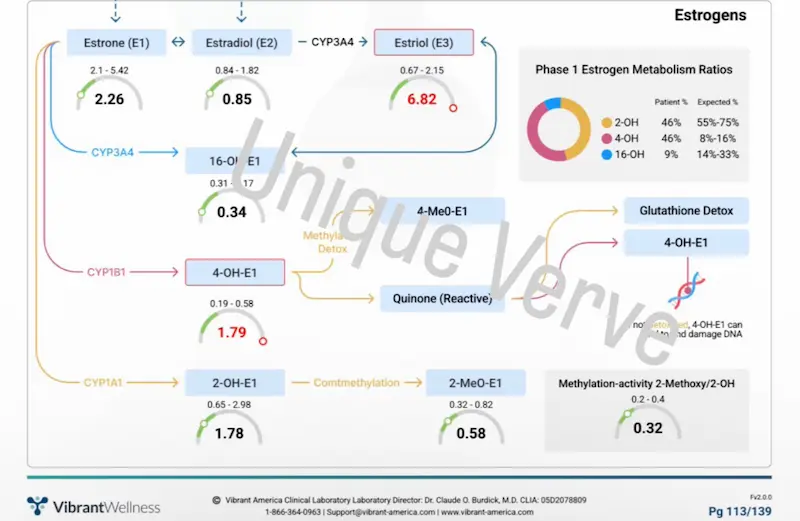
Patient Case 1: High E3 and Elevated 4-OH-E1
My first patient came to me with a constellation of symptoms that had been treated as unrelated for years: life-long constipation, recurrent UTIs, chronic sinus infections, frequent illness and flu, persistent sleep problems, hives, joint pain, significant weight gain and inability to lose weight despite effort, low energy, hair loss, bloating, and water retention. Rosacea was one of many expressions of what was clearly a systemically inflamed body.
Her Vibrant Wellness Hormone Zoomer revealed elevated E3 and high 4-OH-E1 — the DNA-damaging metabolite pattern indicating that her Phase I metabolism was preferentially shunting estrogen through the most unfavorable pathway, and that her Phase II methylation was insufficient to clear it. Her standard hormone blood work had not flagged any of this. Her circulating estrogen levels had not triggered concern. But at the tissue level, her body was generating and accumulating reactive estrogen metabolites that were driving systemic inflammation across every system simultaneously.
Her protocol addressed the full picture: gut restoration and constipation resolution as the prerequisite first step, followed by methylation support, liver detoxification support through the functional medicine detox program, and targeted nutrient repletion. Within three months on the VIP Functional Medicine Program, her symptoms resolved significantly across the board — skin, energy, weight, sleep, immune resilience, and joint pain all improving as the upstream metabolic dysfunction was corrected.
Patient Case 2: Normal Circulating Estrogen, Subclinically High 16-OH, Low 2-OH
My second patient presented with what looked, on paper, like a hormonal mystery. Her E1, E2, and E3 were all within the standard reference range. Standard testing would have sent her home with reassurance that her hormones were fine. But her symptoms related to estrogen dominance told a completely different story: significant bloating, chronic constipation, severe irritability, anxiety, depression, terrible PMS, seasonal allergies, sugar and carbohydrate cravings, hormonal acne, and persistent low energy.
Her Hormone Zoomer revealed the missing piece — and it was not in her circulating estrogen levels but in her Phase I estrogen metabolism ratios. The pie chart told the story immediately: her 2-OH pathway was producing only 39% of her estrogen metabolites against an expected 55–75%. Her 16-OH pathway was running at 43% against an expected 14–33%. And her 4-OH pathway was elevated at 18% against an expected 8–16% — the DNA-damaging metabolite pathway running at more than double its upper expected proportion. Compounding this, her methylation activity marker was flagged in red — indicating that even the 4-OH metabolites being produced were not being adequately methylated and cleared through Phase II, allowing them to accumulate.
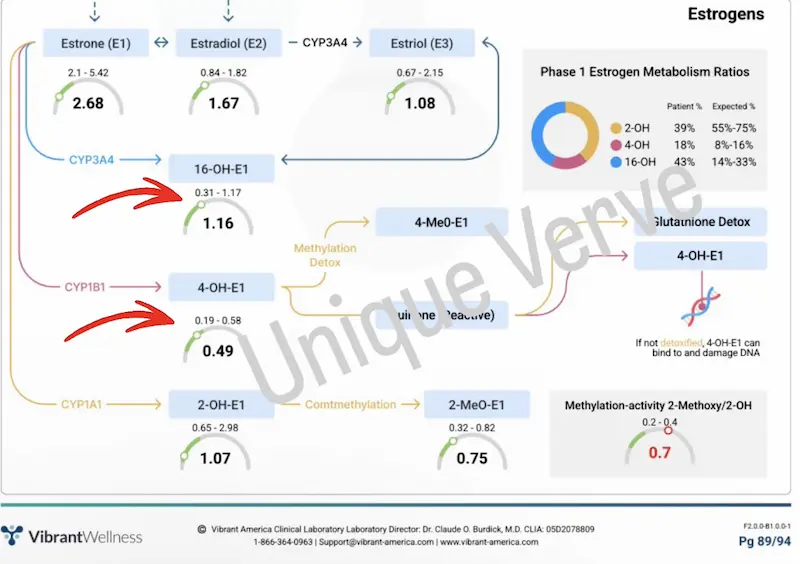
This is the clinical picture that standard blood work structurally cannot see. Her circulating estrogen was normal. Her metabolite distribution was significantly skewed toward both the estrogenic 16-OH pathway and the DNA-damaging 4-OH pathway simultaneously — while her methylation clearance was insufficient to compensate. Her body was not making too much estrogen. It was metabolizing estrogen in the most unfavorable pattern possible, and failing to clear the most harmful byproducts. Her constipation was the key driver — slow transit time was allowing deconjugated estrogen to be reabsorbed, continuously recirculating the estrogenic load and amplifying the metabolite skew regardless of what her production levels showed.
Her protocol began with constipation resolution and gut restoration, followed by 2-OH pathway support through cruciferous vegetable emphasis and targeted supplementation, methylation cofactor repletion to address the impaired Phase II clearance, and lifestyle modifications reducing xenoestrogenic burden. Within three months on the VIP Functional Medicine Program, her PMS, mood, energy, digestion, skin, and cravings had all resolved significantly.
Testing: What I Look For and Why
While every workup is tailored to the individual, the following panels give me the most clinically meaningful picture in poor estrogen clearance cases — and here is why each one matters.
Vibrant Wellness Hormone Zoomer — 24-Hour Urinary Hormone Panel
This is the cornerstone test for estrogen metabolism assessment. Unlike standard hormone blood work which measures circulating hormone levels, the 24-hour urinary panel captures hormone metabolites — showing not just how much estrogen is produced but how it is being metabolized through Phase I and Phase II pathways. Elevated 16-OH-E1 with low 2-OH-E1 indicates preferential metabolism through the estrogenic pathway. Elevated 4-OH-E1 indicates metabolism through the DNA-damaging pathway. Low 2-OHE1:16-OHE1 ratio is a clinically significant finding regardless of whether circulating estrogen levels appear normal. This test reveals what standard blood work structurally cannot.
Micronutrient Panel with SNPs
Cellular levels of methylation cofactors — B2, B6, B9, B12, magnesium — alongside COMT, MTHFR, and other relevant genetic variants. The combination of measured nutrient levels and genetic variants that affect their metabolism is essential for building a precise methylation support protocol. A patient with COMT variants needs a different intervention than a patient with adequate COMT function but B12 depletion — and the micronutrient panel with SNPs provides the specificity to differentiate them.
Gut Zoomer
Comprehensive microbiome assessment including beta-glucuronidase activity, estrobolome health, intestinal permeability markers, and pathogenic burden. Beta-glucuronidase elevation is a direct indicator that the gut is reabsorbing cleared estrogen — making gut restoration and constipation resolution a prerequisite for any liver-level estrogen clearance intervention.
Total Tox Burden
Heavy metals, mycotoxins, and environmental chemicals including xenoestrogenic compounds. Identifying the specific toxic and xenoestrogenic burden informs both the urgency and the specifics of the detoxification protocol — and explains why some patients with otherwise well-supported methylation pathways still show unfavorable estrogen metabolite patterns.
Full Thyroid Panel
TSH, T4, T3, free T3, free T4, reverse T3, and both antibodies. Thyroid function affects gut motility directly — suboptimal thyroid slows transit time and contributes to constipation, which impairs estrogen clearance through the reabsorption mechanism. Thyroid assessment is part of the complete picture in any patient presenting with constipation and estrogen metabolism concerns.
Metabolic Panel and Lipid Panel
Fasting insulin, blood glucose, HbA1c, and liver enzymes. Insulin resistance impairs liver detoxification function and promotes inflammatory dysregulation of Phase I enzymes. Elevated liver enzymes signal detoxification burden. These markers contextualize the estrogen metabolism picture and identify additional modifiable drivers.
The Functional Medicine Approach: Sequencing Matters
While every protocol is individualized to what health history, symptoms and testing reveal, the sequencing principle is consistent across all poor estrogen clearance cases: gut and bowel regularity first, liver support second. This sequencing is not arbitrary — it is clinically essential. Supporting liver detoxification in a patient with constipation and active gut dysbiosis will not produce meaningful estrogen clearance improvement because the cleared estrogen will simply be reabsorbed in the gut. The gut must be addressed first.
Step 1: Gut Restoration and Constipation Resolution
- Mag+Malic (Magnesium Malate) — magnesium supports bowel motility through its osmotic and muscle-relaxing effects, while malate supports mitochondrial energy production. For patients with constipation as a driver of estrogen reabsorption, addressing magnesium status is often the most immediate and impactful first intervention. Magnesium is also a critical methylation cofactor — addressing it simultaneously supports both bowel regularity and Phase II clearance capacity.
- 5-HTP Plus — serotonin is the primary neurotransmitter governing gut motility, and the vast majority of the body’s serotonin is produced in the gut. Constipation is frequently driven by gut dysbiosis impairing serotonin production in enterochromaffin cells, reducing the peristaltic signaling needed for regular bowel movements. 5-HTP provides the direct precursor to serotonin synthesis, supporting motility from the neurochemical level. This connection between gut dysbiosis, serotonin, and constipation is rarely discussed — and it is one of the most clinically meaningful interventions for patients whose constipation has not responded to fiber or hydration alone.
- GI MaxAid — gut lining repair, intestinal barrier restoration, and reduction of beta-glucuronidase activity through microbiome rebalancing.
- Probiotic Integrum — microbiome restoration with clinically selected strains supporting estrobolome health and reducing pathogenic beta-glucuronidase producers.

Step 2: Methylation and Liver Support
Once bowel regularity is established and gut restoration is underway, liver-level estrogen clearance support can be introduced effectively:
- Functional Medicine Detox Program — NutriCleanse GHI (medical food supporting Phase I and Phase II liver detoxification and gut lining integrity) and SulforaOpti (sulforaphane activating the Nrf2 pathway, upregulating Phase II detoxification enzymes, and specifically supporting 2-OH metabolism). Together these provide the most comprehensive liver detoxification support in my dispensary.
- Methylated B-Complex — provides the active forms of B2, B6, B9, and B12 required for COMT function and the broader methylation cycle. Methylated forms are essential for patients with MTHFR variants who cannot efficiently convert standard forms.
- Omega3 BioPure — systemic anti-inflammatory support reducing the inflammatory load on Phase I detoxification enzymes and supporting cell membrane integrity throughout.
Dietary Foundations
The dietary approach for estrogen clearance support focuses on three priorities: removing xenoestrogenic burden by transitioning to organic produce and clean animal products, eliminating conventional dairy and refined carbohydrates that promote insulin resistance and dysbiosis, and specifically emphasizing cruciferous vegetables (broccoli, cauliflower, Brussels sprouts, kale, arugula) which contain indole-3-carbinol and support 2-OH pathway metabolism. These are foundational shifts that create the dietary environment in which supplemental and therapeutic interventions can work most effectively.
Topical Support
The topical approach for skin conditions driven by poor estrogen clearance prioritizes barrier restoration and conservative active support while the internal protocol addresses the root cause. Core recommendations include Environ Pre-Cleansing Oil as a gentle barrier-respecting cleanser suitable across all affected skin conditions including acne, Omega3 BioPure internally as the primary barrier support supplement, Environ’s vitamin A and C-containing moisturizers and serums as tolerated for collagen support and skin structural integrity, and broad-spectrum SPF daily as a non-negotiable. All topical recommendations are condition-specific and individualized.
Your Skin May Be the Most Valuable Signal You Have
If you are struggling with rosacea, hormonal acne, eczema, or any inflammatory skin condition, consider this: your skin may be one of the most valuable diagnostic signals your body has.
Poor estrogen clearance and unfavorable metabolite patterns — particularly elevated 4-OH-E1 — can silently accumulate and contribute to sex hormone-sensitive cancer risk. This risk extends far beyond BRCA genetics. It is shaped by epigenetics, nutrient status, liver function, gut health, toxic burden, lifestyle, and metabolic health — all of which are measurable, and most of which are modifiable. Many women believe that hormonal cancer risk is determined primarily by genetic inheritance. This is a significant and consequential misconception. Your genes load the gun. Your metabolic environment pulls the trigger. And your metabolic environment is something you have substantial influence over.
Many people carry poor estrogen clearance patterns silently for years — with no skin flares, no obvious symptoms, no visible signal — until the downstream consequences become serious. You have something they may not: a visible, external indicator that your body is asking for investigation. The rosacea, the hormonal acne, the skin reactivity that brings you to search for answers is the same internal dysregulation that, addressed now, reduces your long-term risk. It is not a cosmetic problem to manage. It is an opportunity to look upstream, understand what your body is doing with its estrogen at the tissue level, and correct it — for your skin, for your hormonal health, and for your longevity.
This is the foundation of my functional medicine and functional dermatology practice. The skin is the signal. The work is internal. And the testing that reveals it is available to you right now.
The functional medicine approach to poor estrogen clearance does not rely on prescriptions or symptom suppression. It relies on understanding your specific metabolic pattern — and correcting it upstream.
I offer virtual Initial Functional Medicine Health and Skin Assessments for women who are ready to look upstream. This is where we take a full picture of your health history, your current symptoms, and the patterns that connect them — and build a testing and protocol strategy specific to your body.
→ Book your Initial Functional Medicine Health and Skin Assessment
Frequently Asked Questions
What is poor estrogen clearance?
Poor estrogen clearance refers to impaired metabolism and elimination of estrogen through the liver’s Phase I and Phase II detoxification pathways. Rather than being safely metabolized into protective 2-OH metabolites and cleared from the body, estrogen is shunted toward the more estrogenic 16-OH pathway or the DNA-damaging 4-OH pathway. The result is an accumulation of reactive estrogen metabolites that drive systemic inflammation, mast cell activation, and estrogen dominant symptoms — even when circulating estrogen levels appear normal on standard blood work.
Can poor estrogen clearance cause rosacea?
Yes — through multiple interconnected mechanisms. Both the 16-OH and 4-OH estrogen metabolite patterns create functional estrogen dominance that directly stimulates mast cells and increases histamine output, producing the vascular reactivity and flushing characteristic of rosacea. The accumulation of 4-OH reactive metabolites sustains systemic oxidative stress and inflammation that manifests on the skin. And the liver detoxification burden created by poor estrogen clearance impairs the clearance of histamine and other inflammatory mediators simultaneously. Rosacea driven by poor estrogen clearance will not respond fully to topical treatment — the metabolic root cause must be addressed.
How do I know if my estrogen clearance is impaired?
Standard hormone blood work cannot tell you. Blood tests measure circulating estrogen levels — how much your body is producing — but not how that estrogen is being metabolized through Phase I and Phase II liver pathways. The only way to assess estrogen metabolite patterns is through a comprehensive 24-hour urinary hormone panel such as the Vibrant Wellness Hormone Zoomer, which measures E1, E2, E3 alongside their metabolites including 2-OH, 16-OH, and 4-OH fractions. Elevated 4-OH-E1, elevated 16-OH-E1 with low 2-OH-E1, or an unfavorable 2-OH:16-OH ratio are the key findings — all of which can be present alongside completely normal circulating estrogen levels.
What are the symptoms of poor estrogen clearance?
Poor estrogen clearance through the 16-OH pathway produces a highly estrogenic environment that drives: bloating, constipation, severe PMS, irritability, anxiety, depression, sugar and carbohydrate cravings, hormonal acne, eczema, rosacea, weight gain around the hips and abdomen, fluid retention, breast tenderness, and low energy. These are classic estrogen dominance symptoms — and they can all be present with completely normal circulating estrogen levels if the clearance pathway is impaired. Poor clearance through the 4-OH pathway adds systemic oxidative stress, inflammation, and — with chronic accumulation — increased risk of sex hormone-sensitive cancers.
What causes poor estrogen clearance?
The most common drivers I see clinically include: B vitamin and magnesium deficiencies impairing methylation; COMT and MTHFR genetic variants reducing Phase II enzyme activity; gut dysbiosis elevating beta-glucuronidase and allowing cleared estrogen to be reabsorbed; constipation increasing transit time and estrogen reabsorption opportunity; alcohol depleting methylation cofactors and impairing liver detoxification; xenoestrogens from conventional produce, dairy, plastics, and personal care products adding estrogenic burden; insulin resistance and chronic stress impairing Phase I detoxification; and an insufficient intake of cruciferous vegetables that support the protective 2-OH pathway.
Can you have estrogen dominance with normal estrogen levels?
Yes — and this is one of the most important and most frequently missed clinical realities in hormonal health. Estrogen dominance is not solely determined by how much estrogen you produce. It is also determined by how that estrogen is metabolized and cleared. A woman with normal circulating E1, E2, and E3 who preferentially metabolizes estrogen through the highly estrogenic 16-OH pathway will experience a full picture of estrogen dominance symptoms despite normal blood work. Standard hormone testing will not identify this pattern. A 24-hour urinary hormone panel that measures estrogen metabolites is the only way to see it.
Does estrogen clearance affect cancer risk?
Research has specifically implicated elevated 4-OH-E1 — the DNA-damaging estrogen metabolite — in the initiation of sex hormone-sensitive cancers including breast cancer, through the formation of DNA adducts in hormone-sensitive tissue. This is an independently modifiable risk factor that extends well beyond BRCA genetic status. Many women believe hormonal cancer risk is primarily determined by BRCA genetics. In reality, how your body metabolizes and clears estrogen — shaped by nutrient status, liver function, gut health, toxic burden, and lifestyle — is a significant and correctable part of the risk picture. Identifying and addressing unfavorable estrogen metabolite patterns through comprehensive testing is an act of genuine cancer risk reduction.
Why does constipation affect estrogen clearance?
The liver processes estrogen and prepares it for excretion through bile into the digestive tract. In the gut, certain bacteria produce beta-glucuronidase — an enzyme that deconjugates estrogen that has already been cleared by the liver, allowing it to be reabsorbed into circulation. When transit time is slow due to constipation, this reabsorption window is extended and the recirculating estrogenic load increases. This is why addressing constipation is always the first priority in a poor estrogen clearance protocol — liver support introduced before bowel regularity is established will not produce meaningful clearance improvement because the gut will continue to reabsorb what the liver has processed.
Why is my rosacea worse when my hormones change?
Because hormonal shifts — particularly those involving estrogen fluctuation — directly affect mast cell behavior and histamine output. Estrogen stimulates mast cells, and when estrogen levels surge or fluctuate erratically (as they do in the luteal phase of the menstrual cycle, during perimenopause, or after stopping birth control), mast cell degranulation increases and rosacea flares follow. But the more important question is why your mast cells are reactive enough for normal hormonal fluctuations to produce an outsized skin response. That reactivity reflects the underlying internal picture — including how your estrogen is being metabolized and cleared, not just how much is circulating. Poor clearance through the 16-OH or 4-OH pathways amplifies mast cell sensitivity even when estrogen levels appear within normal range.
Is my rosacea hormonal or environmental?
Almost always both — and the distinction matters less than identifying which specific internal and external drivers are active in your body. Hormonal drivers (estrogen dominance, poor clearance, progesterone decline, cortisol dysregulation) lower the threshold at which your skin reacts to environmental triggers (UV, heat, wind, certain topical ingredients). When the hormonal picture is addressed — when estrogen is being metabolized favorably, mast cells are stabilized, and histamine is being cleared efficiently — environmental triggers that previously caused significant flares often become manageable or stop triggering responses entirely. The environmental sensitivity is frequently a downstream expression of the hormonal and metabolic vulnerability, not an independent problem requiring separate management.
Is rosacea permanent or can it get better?
Rosacea can improve significantly — and for many of my patients, it resolves to the point where it is no longer a daily management concern. Whether it improves, and how much, depends entirely on whether the upstream internal drivers are identified and addressed. When mast cell activation, poor estrogen clearance, gut dysbiosis, food sensitivities, thyroid dysfunction, and nutrient insufficiency are corrected systematically, the internal inflammatory environment that sustains rosacea is no longer present — and the skin reflects that. Topical management and trigger avoidance alone rarely produce lasting improvement because they do not change the internal conditions driving reactivity. A root-cause functional medicine approach aims for resolution, not indefinite management.
Written by Natalie Maibenko – a Certified Functional Medicine Practitioner and Master Esthetician with 22+ years of experience and founder of Unique Verve

As a Certified Functional Medicine Practitioner my Expertise Encompasses:
- Immune System: frequent illness, UTIs, yeast infections
- Allergies, Asthma
- Skin Problems: acne, cystic acne, rosacea, eczema, dermatitis, ichthyosis, psoriasis, vitiligo, melasma
- Inflammation: arthritis, rhinitis, joint & muscle pain, migraines, headaches
- Sleep Disturbunces, Insomnia
- Gut Problems: IBS/IBD, bloating, acid reflux, gas, constipation, diarrhea, parasites, fungal/yeast overgrowths
- Hormonal Imbalances: PCOS, PMS symptoms, weight problems/inability to lose weight, thyroid problems
- Hair Loss, Alopecia
- Mood Imbalances: anxiety, depression, irritability
- Metabolic Dysfunction, Insulin Resistance, Type 2 Diabetes
- Optimizing Wellness for Successful Pregnancy
- Autoimmune Conditions: Hashimoto’s thyroiditis, grave’s disease, reumatoid arthritis (RA), lupus, etc
- Bone Health: osteopenia/ osteoporosis
- Effective Anti-Aging Strategies without Injectables with the inside-out & outside-in approach
- Detoxification of Heavy Metals, Mycotoxins, Environmental Toxins
- Reversing Breast Implant Illness
- Preparation for the Explant Surgery and Optimization of Wellness & Vitality Post-Explant
With love and gratitude,
Natalie Maibenko
Functional Medicine & Skincare Expert – Helping You Take Control of Your Health and Achieve Lasting Skin Results Nationwide — Virtual Practice
Disclaimer: Information and content on this website is provided for educational purposes only, and is not intended to diagnose, treat and to be a substitute for the advice provided by your physician or other healthcare professional. No information offered here should be interpreted as a diagnosis of any disease, nor an attempt to treat or prevent or cure any disease or condition. If you have any concerns or questions about your health, you should always consult with a physician or other healthcare professional. Do not disregard, avoid, or delay obtaining medical or health-related advice from your healthcare professional. Always speak with your healthcare professional before taking any medications, supplements or pursuing any wellness programs. Information provided on this website does not create a doctor-patient relationship between you and any professional affiliated with this website.