Introduction
Is rosacea caused by Demodex mites? It is one of the most searched questions in the rosacea community — and the answer is more nuanced, and more clinically important, than most dermatology offices explain. Demodex mites appear together with rosacea consistently enough that the connection is real. But the critical question is not whether Demodex is causing your rosacea — it is why your immune system lost its ability to regulate a mite that lives on virtually every adult’s skin without causing problems.
If you have been down this path and found that the skin improvement was temporary — or that the treatment irritated your already reactive rosacea skin — what you experienced is the predictable consequence of treating a symptom without asking the more important question: why did the Demodex overgrow in the first place?
Demodex mites are not foreign invaders. They are normal inhabitants of human skin — present in virtually every adult, living in hair follicles and sebaceous glands, existing in balance with the immune system under healthy conditions. The question that conventional dermatology rarely asks is not how to eliminate them, but why the immune system lost its ability to regulate them. That upstream question is where the real clinical story begins — and where lasting resolution is found.
In my functional medicine and functional dermatology practice, Demodex overgrowth is never the diagnosis. It is the signal — a visible, measurable expression of an immune system that has been weakened by specific, identifiable, and addressable upstream drivers. Understanding what those drivers are, how they interconnect, and why addressing them resolves Demodex overgrowth without a single topical mite treatment is what this post is about.
This post is written for the reader who is encountering this clinical picture for the first time — who may have just received a Demodex diagnosis or discovered through her own research that mites might be contributing to her rosacea, and who wants to understand what is actually driving the overgrowth and what a genuine root-cause approach looks like. Every protocol I build is individualized to what your specific health history and testing reveal — what follows is the clinical framework I work within.
What Is Demodex — And Why Does Everyone Have It?
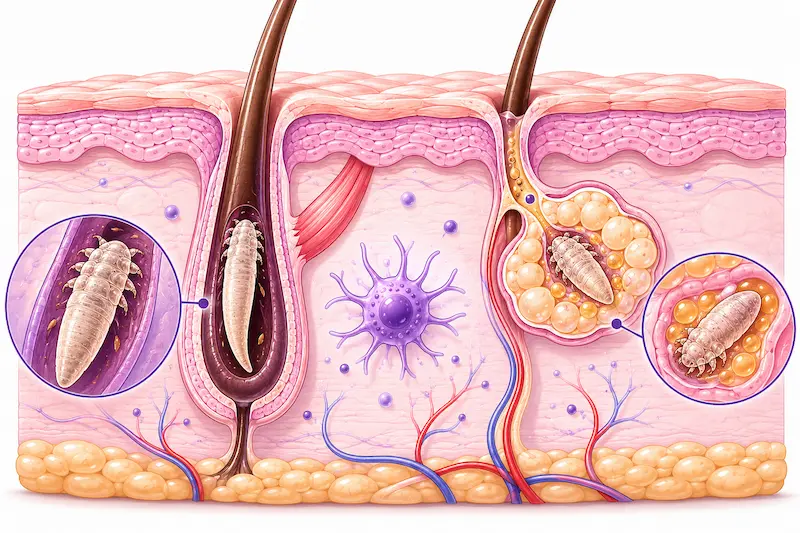
So is rosacea caused by Demodex mites? Research consistently finds higher Demodex density in rosacea patients compared to the general population — in some studies nearly six times higher. The connection is real and clinically significant. But the more precise answer is that Demodex overgrowth is a marker and amplifier of rosacea, not its sole primary cause. Demodex is a genus of microscopic mite with two species relevant to human skin: Demodex folliculorum, which lives in hair follicles, and Demodex brevis, which lives in sebaceous glands. Both are obligate parasites — they can only survive on human skin — and both are extraordinarily common. Studies consistently find Demodex present in virtually all adults over 18, with prevalence increasing with age.
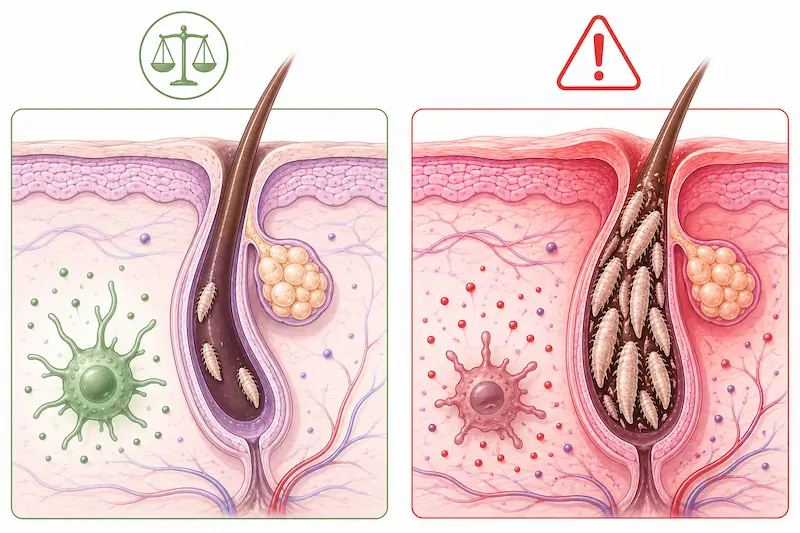
Under normal immune conditions, Demodex populations are small, stable, and clinically insignificant. Langerhans cells — the immune sentinels of the skin — maintain tolerance to Demodex as a normal skin inhabitant, preventing the immune system from mounting an inflammatory response to a benign commensal. This immune tolerance is the key concept: Demodex does not cause rosacea because it exists. It causes rosacea when the immune system stops tolerating it.
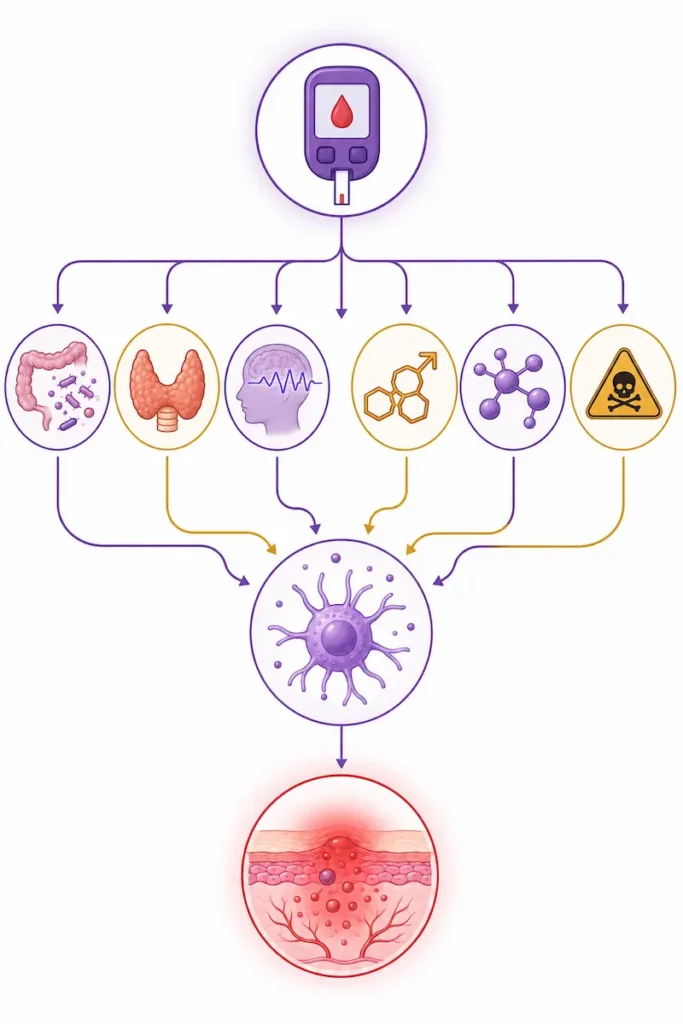
When Langerhans cell function is impaired — by blood sugar dysregulation, gut dysbiosis, thyroid dysfunction, nutrient insufficiency, toxic burden, cortisol dysregulation, or hormonal imbalance — the normal tolerance mechanism breaks down. Demodex populations are no longer kept in check. The mites proliferate in the follicle environment, their waste products and dying cells trigger an inflammatory immune response, and the characteristic redness, flushing, papules, and pustules of rosacea intensify or appear for the first time.
Demodex overgrowth in rosacea is therefore not a primary skin infection. It is secondary evidence of a compromised immune environment — evidence that something upstream has weakened the skin’s immune regulation capacity to the point where a normal skin inhabitant has become an inflammatory trigger.
Is Rosacea Caused by Demodex Mites? Understanding the Upstream Drivers
Understanding why Demodex overgrows requires understanding what creates the internal environment that allows it. The following drivers are the most clinically significant — and they do not operate independently. They feed each other, creating a compounding cascade that progressively weakens immune regulation and creates increasingly favorable conditions for Demodex proliferation.
1. Blood Sugar Dysregulation — The Primary Driver
Elevated blood glucose levels and poor glycemic control are the most clinically significant upstream drivers of Demodex overgrowth — and the most consistently overlooked. Research specifically links high blood sugar to significantly increased risk of severe facial and ocular Demodex infestation, including Demodex blepharitis.
The mechanisms are multiple and interconnected. Elevated blood glucose directly creates an ideal nutrient-rich environment in which Demodex mites thrive — the glucose-rich sebaceous secretions feed the mite population and accelerate proliferation. Blood sugar dysregulation simultaneously impairs immune cell function, reducing the Langerhans cell activity needed to maintain Demodex tolerance and regulation.
The ATP connection adds a critically important dimension that is almost never discussed in consumer-facing content. Intracellular ATP (adenosine triphosphate) plays a dual role in Demodex overgrowth: low host ATP — which occurs when blood sugar dysregulation impairs mitochondrial energy production — produces a poor immune response that allows Demodex to overpopulate unchecked. Simultaneously, ATP released from dying cells acts as a danger signal that drives the resulting skin inflammation and immune hypersensitivity response. Blood sugar dysregulation therefore both enables the overgrowth and amplifies the inflammatory response it produces. This mast cell activation and the histamine cascade it produces is explored in depth in our post on the histamine-rosacea gut connection — a parallel pathway that frequently co-exists with Demodex overgrowth in treatment-resistant rosacea.
High blood sugar is also directly corrosive to tissue integrity — including the acid mantle of the skin. A compromised acid mantle reduces the skin’s primary chemical defense against microbial overgrowth, creating a more permissive surface environment for Demodex proliferation alongside the impaired immune regulation happening internally.
Blood sugar dysregulation does not occur in isolation. It drives gut dysbiosis by feeding pathogenic bacteria and disrupting the microbiome. It impairs thyroid function through glycation of thyroid hormone receptors and conversion enzymes. It depletes intracellular nutrients through increased urinary excretion and impaired cellular uptake. Every other upstream driver of Demodex overgrowth is amplified by poor glycemic control — which is why it sits at the top of the clinical picture.
2. Gut Dysbiosis and Impaired Immune Regulation
The gut microbiome is the primary regulator of systemic immune function — and a disrupted gut microbiome directly impairs the immune surveillance capacity that keeps Demodex populations in check. Gut dysbiosis reduces the production of short-chain fatty acids that modulate immune cell behavior, impairs the regulatory T cell populations that maintain immune tolerance, and drives systemic inflammation through LPS translocation that shifts the immune environment toward reactivity rather than regulation.
In patients with Demodex overgrowth, gut dysbiosis is almost always part of the picture. The same leaky gut that allows bacterial fragments into circulation also impairs the mucosal immune regulation that, through systemic immune crosstalk, affects Langerhans cell function in the skin. A gut that is chronically inflamed produces an immune system that is chronically reactive — and a chronically reactive immune system cannot maintain the nuanced tolerance that Demodex regulation requires.
Parasitic infection adds a specific dimension. Parasites directly suppress immune function as a survival strategy — impairing the very immune cells responsible for regulating Demodex populations. In patients with concurrent parasitic burden and Demodex overgrowth, the parasitic immune suppression is frequently a central driver of why the Demodex cannot be regulated even when other interventions are in place. Importantly, standard stool tests do not always detect parasites even when levels are clinically significant — which is why comprehensive testing that goes beyond standard panels is essential when parasitic burden is suspected.
3. Thyroid Dysfunction
Suboptimal thyroid function impairs immune competence through multiple mechanisms — reducing the activity and proliferation of immune cells, slowing the gut motility that prevents dysbiosis, and impairing the cellular energy production (ATP synthesis) needed for immune cell function. When thyroid function is suboptimal, the immune system operates at reduced capacity across every dimension — including the Langerhans cell surveillance that regulates Demodex populations in the skin.
Thyroid dysfunction and blood sugar dysregulation create a particularly powerful compounding interaction in the context of Demodex. Hypothyroidism reduces cellular glucose uptake and impairs insulin sensitivity, worsening blood sugar dysregulation. Poor blood sugar control in turn impairs thyroid hormone conversion and receptor function. Together they create a metabolic environment of reduced cellular energy, impaired immune function, and progressive loss of the regulatory capacity that keeps Demodex in check.
4. Cortisol Dysregulation and Chronic Stress
Scientific research establishes a clear mechanistic link between cortisol dysregulation and Demodex overgrowth. Stress-induced cortisol elevation suppresses the immune system through multiple pathways — reducing lymphocyte activity, impairing Langerhans cell function, and altering the skin’s barrier integrity in ways that create a more permissive environment for Demodex proliferation.
Chronically elevated cortisol reduces the skin’s natural defense mechanisms at exactly the surface level where Demodex regulation occurs — impairing the acid mantle, altering sebaceous secretion composition, and reducing the antimicrobial peptide production that helps regulate follicular populations. For women in perimenopause — who are already managing HPA axis dysregulation alongside declining reproductive hormones — the cortisol burden on immune regulation is significant and directly relevant to Demodex overgrowth risk.
5. Hormonal Imbalance and Androgen-Driven Sebum
Research establishes a strong bidirectional link between hormonal imbalances and Demodex proliferation. Androgens — particularly testosterone and its more potent derivative DHT — directly regulate sebaceous gland activity and sebum production. Sebum is the primary food source for Demodex mites. An androgen-driven increase in sebum output creates the lipid-rich follicular microenvironment in which Demodex thrives.
In perimenopausal women, this dynamic is particularly relevant. As estrogen and progesterone decline, androgens can become relatively dominant — not necessarily because testosterone is absolutely elevated, but because the hormonal balance has shifted. DHT is often the more clinically significant androgen in this picture, as it is a more potent driver of sebaceous activity than testosterone itself. In late perimenopause and beyond, androgen dominance becomes increasingly common and represents a direct nutritional contribution to Demodex overgrowth through sebum amplification.
Conversely, Demodex mites and their waste products trigger localized immune responses that can drive further systemic inflammation — creating a bidirectional loop in which hormonal imbalance feeds Demodex, and Demodex amplifies the inflammatory environment that worsens hormonal dysregulation.
6. Nutrient Insufficiencies
The immune cells responsible for Demodex regulation — including Langerhans cells and regulatory T cells — require specific nutrient cofactors to function. Zinc is essential for immune cell development and skin barrier integrity. Vitamin A regulates epithelial cell turnover and immune function in the skin directly. Vitamin D modulates immune tolerance and reduces the inflammatory reactivity that drives hypersensitivity responses. B vitamins support the cellular energy production needed for immune cell activity.
When these nutrients are depleted — through poor absorption driven by gut dysbiosis, through chronic stress increasing metabolic demand, through blood sugar dysregulation increasing urinary excretion, or through genetic variants affecting metabolism — the immune infrastructure needed for Demodex regulation is progressively undermined. Nutrient insufficiency is rarely the primary driver of Demodex overgrowth, but it is consistently a compounding factor that makes every other upstream driver harder to correct.
7. Toxic Burden
Environmental toxins — heavy metals, mycotoxins, and endocrine-disrupting compounds — suppress immune function directly and compound every other upstream driver of Demodex overgrowth. Toxic burden impairs mitochondrial ATP production, reducing the cellular energy available for immune surveillance. It impairs thyroid function through receptor competition and enzyme inhibition. It worsens blood sugar dysregulation through insulin receptor interference. And it directly suppresses Langerhans cell activity — the primary skin immune sentinel responsible for Demodex regulation.
In patients where Demodex overgrowth persists despite addressing other upstream drivers, toxic burden is frequently the missing variable. It is also one of the most commonly overlooked — because it requires specific testing to identify and is not part of any standard dermatological or even general medical workup.
When Demodex Goes Beyond the Skin: Ocular Involvement as a Systemic Signal
Demodex folliculorum colonizes not only facial hair follicles but also the eyelash follicles and meibomian glands of the eyelids. When Demodex overpopulates in the ocular region — driven by the same upstream immune dysregulation driving facial rosacea — it produces a condition called Demodex blepharitis: chronic inflammation of the eyelid margins characterized by lid redness and swelling, a gritty or foreign body sensation in the eye, crusting or collarettes at the base of the eyelashes, blurry vision, light sensitivity, and chronic styes or chalazia.
Ocular Demodex is significantly underdiagnosed — in part because patients and practitioners do not connect chronic eye symptoms to a skin condition, and in part because the mites are microscopic and require specific examination to identify. Many women managing rosacea for years have concurrent Demodex blepharitis that has never been identified or connected to their skin picture.

The clinical significance of ocular Demodex involvement extends beyond the eye symptoms themselves. When Demodex has established in both the facial skin and the ocular region simultaneously, it is a signal that the underlying immune dysregulation is systemic and significant — not localized to a single skin area. The same blood sugar dysregulation, gut immune impairment, thyroid dysfunction, and cortisol burden that allowed facial Demodex to overgrow has created a permissive environment throughout the mucosal and epithelial surfaces of the face and eyes. Ocular involvement is the immune system’s way of indicating that the upstream picture requires comprehensive investigation — not more targeted topical treatment.
Research specifically links elevated blood glucose to significantly increased risk of severe ocular Demodex infestation. For women with rosacea who also experience chronic eye irritation, lid inflammation, or recurring styes — glycemic assessment is a clinically important and frequently omitted step.
Why Conventional Demodex Treatment Keeps Failing
The standard conventional approach to Demodex rosacea includes topical ivermectin (Soolantra), oral ivermectin in more severe cases, topical permethrin, metronidazole, and — particularly in natural health circles — tea tree oil (terpinen-4-ol) preparations. Each of these targets the mite directly. None of them addresses why the immune system lost its ability to regulate Demodex in the first place.
The result is a predictable pattern: treatment reduces the Demodex population temporarily, the skin improves, treatment ends or the mite develops tolerance, the upstream immune dysregulation remains unchanged, Demodex repopulates from the surviving population or from re-exposure, and the rosacea returns. This cycle repeats — often with diminishing returns from each subsequent treatment course — because the conditions enabling the overgrowth have not been corrected.
Tea tree oil deserves specific attention because it is so widely recommended in the natural health space and carries a particular risk for the rosacea patient. Tea tree oil is cytotoxic to Demodex at therapeutic concentrations — it can reduce mite populations. But for a woman with rosacea whose skin barrier is already compromised, whose acid mantle is already disrupted, and whose skin is already in a state of heightened reactivity, applying a concentrated essential oil is actively counterproductive. Tea tree oil at concentrations effective against Demodex is significantly irritating to sensitized skin — it damages the barrier it is applied to, increases skin reactivity, and worsens the inflammatory picture it is meant to address. Reducing the Demodex count while simultaneously damaging the skin barrier is not a net clinical benefit. It is trading one problem for another while leaving the root cause entirely unaddressed.
The fundamental error of conventional Demodex treatment — whether pharmaceutical or natural — is the same as the fundamental error of conventional rosacea treatment broadly: treating the visible manifestation without investigating the internal environment that produced it. Demodex is not the disease. It is the signal. And signals require investigation, not suppression.
A Patient Story: When the Immune System Reclaims Control
One of my patients came to me with rosacea that had not responded meaningfully to conventional treatment. Her internal picture was significant: her testing revealed clinically elevated fasting insulin — confirming the blood sugar dysregulation that is so consistently at the center of Demodex cases — alongside high levels of detectable parasites on her comprehensive stool test, Gut Zoomer as well as eosinophil count on her basic lab test panel. It is worth noting that standard stool tests frequently fail to detect parasites even when levels are clinically significant — her parasite burden was substantial enough to be clearly identified, which underscored the degree of immune suppression she was experiencing.
Her symptom picture extended well beyond her skin: daily loose stools, gas, bloating, and acid reflux reflecting the gut dysfunction driving her immune dysregulation; depression, irritability, and poor sleep reflecting the systemic inflammatory and neurotransmitter consequences of chronic gut infection and blood sugar instability; and persistent sugar and refined carbohydrate cravings — a direct clinical signal of blood sugar dysregulation and the gut dysbiosis feeding it.
Her protocol addressed the upstream picture systematically — blood sugar regulation, parasitic and gut infection clearance, gut restoration, thyroid and immune support. She did not treat Demodex directly at any point.
After three months on the functional medicine program, her mood and sleep had improved significantly. Her bowel movements normalized. The acid reflux, gas, and bloating resolved. Her energy and mental clarity returned. Five months after beginning the protocol — without any topical anti-Demodex treatment — she underwent microscopic examination of her skin. Her Demodex count had normalized. The mites were no longer detectable at overgrowth levels.
This outcome is not surprising from a functional medicine perspective — it is the expected consequence of restoring the upstream immune competence that Demodex regulation requires. When the internal environment no longer supports overgrowth, and when the immune system has regained the capacity to regulate its skin inhabitants, Demodex returns to its normal commensal status without being directly targeted. The skin clears because the body reclaimed control — not because the mite was killed.
The Functional Medicine Approach: Restoring the Upstream Environment
The functional medicine approach to Demodex rosacea does not begin with the mite. It begins with the question every conventional treatment skips: what has weakened the immune system’s ability to regulate a normal skin inhabitant?
The answer is always individual. Blood sugar dysregulation may be the primary driver in one patient. Gut dysbiosis with parasitic burden may be central in another. Thyroid dysfunction creating the metabolic environment for immune impairment may be the upstream correction that makes everything else possible. Androgen-driven sebum excess feeding the mite population may need to be addressed alongside gut and immune restoration. Toxic burden may be the hidden suppressor that prevents immune recovery despite addressing other factors. Nutrient insufficiency may be the limiting factor that keeps the immune infrastructure from functioning even when the infections are cleared.
Every protocol is built around what your specific health history, symptom picture, and comprehensive testing reveal. The upstream drivers are identified individually. The interventions are sequenced based on what needs to be addressed first in your specific case. And the outcome — immune restoration and Demodex regulation — follows from correcting the environment, not from targeting the mite.
This is not a faster approach than conventional treatment. It is a more complete one. And it is the only approach that addresses why Demodex overgrew in the first place — which is the only way to prevent it from returning.
Is Rosacea Caused by Demodex Mites? The Answer That Changes Everything
In order to find true healing and resolution, we need to address the upstream root causes and drivers. And because everyone is different — because your blood sugar picture, your gut health, your thyroid, your hormones, your toxic burden, and your nutrient status are uniquely yours — the protocol must be built around your specific case.
Tea tree oil will not fix blood sugar dysregulation. Ivermectin will not restore gut immune function. Permethrin will not correct thyroid dysfunction or rebalance androgens. None of these treatments can restore the Langerhans cell tolerance that Demodex regulation requires — because none of them touch the upstream environment that destroyed it.
If your rosacea has a Demodex component — whether diagnosed by a dermatologist or suspected through your own research — the most important step you can take is not finding a more effective mite treatment. It is finding out why your immune system lost its ability to regulate a mite it has coexisted with for your entire adult life. That investigation is where the answers are. And those answers are different for every person.
This is the foundation of my functional medicine and functional dermatology practice. The skin is the signal. The work is internal. And the protocol is yours — built around your unique case, your health history, and your specific upstream drivers.
→ Book your Initial Functional Medicine Health and Skin Assessment
Frequently Asked Questions
Q1: What is Demodex rosacea?
Demodex rosacea refers to rosacea in which an overgrowth of Demodex mites — microscopic organisms that normally inhabit human skin in small, regulated populations — is contributing to facial inflammation. Demodex mites are present in virtually all adults and are normally tolerated by the skin’s immune system. When the immune system loses its regulatory capacity — due to blood sugar dysregulation, gut dysbiosis, thyroid dysfunction, hormonal imbalance, cortisol dysregulation, nutrient insufficiency, or toxic burden — Demodex populations overgrow and their presence triggers an inflammatory response that intensifies rosacea. Demodex overgrowth is not the root cause of rosacea. It is a signal of impaired immune regulation with specific, identifiable upstream drivers.
Q2: How do I know if Demodex is causing my rosacea?
Demodex rosacea is typically characterized by rosacea that has not responded well to conventional treatment, worsening of redness and pustules particularly around the nose, cheeks, and forehead, a sensation of something crawling or moving in the skin (reported by some patients), and concurrent eye symptoms such as lid inflammation, gritty sensation, or recurring styes suggesting ocular Demodex involvement. Definitive identification requires microscopic examination of follicular material. However, the more clinically important question is not whether Demodex is present in elevated numbers — it almost certainly is if conventional rosacea treatment has failed — but what upstream drivers have compromised the immune regulation that should be keeping it in check.
Q3: Does tea tree oil kill Demodex?
Tea tree oil (specifically terpinen-4-ol) is cytotoxic to Demodex at therapeutic concentrations and can reduce mite populations. However, for rosacea patients whose skin barrier is already compromised and whose skin is in a state of heightened reactivity, tea tree oil at concentrations effective against Demodex is significantly irritating and can worsen the barrier damage and inflammatory response it is intended to address. More critically, tea tree oil does not address any of the upstream drivers — blood sugar dysregulation, gut dysbiosis, thyroid dysfunction, hormonal imbalance — that allowed Demodex to overgrow in the first place. Reducing the mite count while leaving the root cause unaddressed produces temporary improvement at best and barrier damage at worst.
Q4: Can Demodex affect my eyes?
Yes — Demodex folliculorum colonizes eyelash follicles and meibomian glands as well as facial hair follicles. Ocular Demodex overgrowth produces Demodex blepharitis: chronic eyelid margin inflammation with symptoms including lid redness, gritty or foreign body sensation, crusting at the base of eyelashes, blurry vision, light sensitivity, and recurring styes. Ocular involvement alongside facial rosacea is a signal that the underlying immune dysregulation is systemic and significant. Research specifically links elevated blood glucose to increased risk of severe ocular Demodex infestation — making glycemic assessment an important and frequently overlooked step in patients with concurrent rosacea and chronic eye symptoms.
Q5: Why does Demodex keep coming back after treatment?
Because treatment targeted the mite without addressing the upstream immune environment that allowed it to overgrow. Ivermectin, permethrin, and tea tree oil can reduce Demodex populations temporarily — but when the internal drivers of immune dysregulation remain unchanged, the conditions for Demodex overgrowth persist. Mites repopulate from surviving organisms or re-exposure, the immune system remains unable to regulate them, and the rosacea returns. Lasting resolution requires identifying and correcting the specific upstream drivers — blood sugar dysregulation, gut dysbiosis, thyroid dysfunction, hormonal imbalance, cortisol burden, nutrient insufficiency, toxic burden — that compromised immune regulation in the first place.
Q6: What is the connection between blood sugar and Demodex?
Blood sugar dysregulation is one of the most clinically significant and most overlooked drivers of Demodex overgrowth. Elevated blood glucose creates a nutrient-rich environment that directly feeds Demodex mite populations and accelerates proliferation. It impairs the immune cell function needed to regulate Demodex populations. It reduces intracellular ATP production — and low host ATP produces a poor immune response that allows Demodex to overpopulate unchecked, while ATP released from dying cells drives the resulting skin inflammation. And it drives gut dysbiosis, thyroid dysfunction, and nutrient insufficiency — amplifying every other upstream driver of Demodex overgrowth simultaneously. Glycemic assessment is one of the most important and most frequently omitted steps in a comprehensive Demodex rosacea workup.
Q7: Can fixing my gut help with Demodex rosacea?
Yes — significantly. The gut microbiome is a primary regulator of systemic immune function, including the Langerhans cell activity in the skin that maintains Demodex tolerance and regulation. Gut dysbiosis reduces the immune regulatory capacity needed to keep Demodex populations in check, drives systemic inflammation through LPS translocation, and creates the impaired immune environment in which Demodex overgrowth is sustained. Parasitic infection — which is often concurrent with Demodex overgrowth and is frequently missed on standard stool testing — directly suppresses the immune cells responsible for Demodex regulation. Restoring gut health and clearing gut infections restores the systemic immune competence that Demodex regulation requires.
Q8: Is Demodex rosacea contagious?
Demodex mites can be transmitted through close skin contact — they are found on virtually all adults and transmission between people is normal and unavoidable. However, Demodex rosacea is not contagious in the conventional sense, because the clinical problem is not the presence of the mites — it is the loss of immune regulation that allows them to overgrow. A person with healthy immune regulation exposed to Demodex will simply maintain normal mite populations. A person with compromised immune regulation from blood sugar dysregulation, gut dysbiosis, or other upstream drivers will be unable to regulate the mites regardless of exposure source. The mites are not the disease. The compromised immune environment is.
Q9: How do I know if I have Demodex mites?
Demodex overgrowth does not produce a single identifiable symptom — it overlaps significantly with general rosacea presentation. Signs that Demodex may be a contributing factor include rosacea that has not responded to conventional treatment, worsening of papules and pustules particularly around the nose and cheeks, a rough or sandpaper-like skin texture between flares, a crawling or itching sensation in the skin reported by some patients, and concurrent eye symptoms such as lid inflammation, gritty sensation, or recurring styes. Definitive identification requires microscopic examination of follicular material. However the more clinically important question is not whether Demodex is elevated, but why the immune system lost its capacity to regulate it — because that upstream answer is what determines the protocol.
Q10: Can Demodex mites spread to my eyes?
Yes — Demodex folliculorum colonizes eyelash follicles and meibomian glands as readily as facial hair follicles. When Demodex overpopulates in the ocular region it produces Demodex blepharitis: chronic eyelid margin inflammation with symptoms including lid redness, gritty or foreign body sensation, crusting at the lash base, blurry vision, light sensitivity, and recurring styes or chalazia. Ocular involvement alongside facial rosacea is clinically significant — it signals that the underlying immune dysregulation is systemic rather than localized to the facial skin. Research specifically links elevated blood glucose to increased risk of severe ocular Demodex infestation, making glycemic assessment a particularly important step for any patient presenting with both facial rosacea and chronic eye symptoms.
Q11: Why did my dermatologist miss my Demodex?
Because diagnosing Demodex requires a microscopic examination of follicular material — a procedure that is not part of a standard dermatology assessment for rosacea. Most dermatologists diagnose rosacea visually based on presentation pattern and manage it with topical or oral treatments without investigating whether Demodex overgrowth is a contributing factor. Additionally, because Demodex is present in low numbers on virtually all adult skin, the distinction between normal colonization and pathological overgrowth requires quantification rather than simply detection — a nuance that is easy to miss without specific testing intent. From a functional medicine perspective, even identifying Demodex overgrowth is only the beginning of the relevant clinical question — the more important investigation is what upstream immune dysregulation allowed it to develop.
Q12: Does everyone with rosacea have Demodex mites?
Everyone has Demodex mites — they are present in virtually all adults regardless of whether they have rosacea. The clinical question is not whether Demodex is present but whether it is present in elevated numbers, and whether its presence is contributing to the inflammatory picture. Research consistently finds higher Demodex density in rosacea patients compared to controls — but not all rosacea is Demodex-driven, and not all Demodex overgrowth produces the same presentation. Demodex is one of several potential contributors to rosacea, alongside gut dysbiosis, histamine overload, estrogen dominance, poor estrogen clearance, H. Pylori, and SIBO. Whether it is a central driver in your specific case depends on your individual clinical picture — which is why comprehensive assessment rather than assumption is the appropriate starting point.
Q13: What triggers Demodex mite overgrowth?
Demodex overgrowth is triggered by the loss of immune regulation — specifically the impairment of Langerhans cell function in the skin that normally keeps Demodex populations in check. The upstream drivers that impair this immune regulation include blood sugar dysregulation (the most clinically significant, creating both a nutrient-rich environment for mite proliferation and impaired immune surveillance), gut dysbiosis and parasitic infection suppressing systemic immune function, suboptimal thyroid function reducing immune competence, cortisol dysregulation impairing skin barrier defenses, relative androgen dominance increasing sebum production and creating the lipid-rich follicular environment Demodex feeds on, nutrient insufficiencies depleting the immune infrastructure, and toxic burden suppressing Langerhans cell activity. These drivers compound each other — which is why Demodex overgrowth is almost always a multi-factor picture requiring comprehensive investigation.
Q14: Is my rosacea actually a parasite problem?
Demodex mites are technically classified as parasites — they are obligate parasites that can only survive on human skin. However framing rosacea as a parasite problem misses the more important clinical reality: Demodex overgrowth is a consequence of impaired immune regulation, not a primary infection in the conventional sense. A healthy immune system coexists with Demodex without issue. The parasitic burden I assess in rosacea patients through comprehensive gut testing — including H. Pylori, intestinal parasites, and SIBO — is a separate and equally important clinical dimension: gut parasitic infections suppress the systemic immune function that regulates Demodex on the skin. Addressing gut parasitic burden as part of restoring immune competence is frequently one of the most impactful upstream interventions in treatment-resistant rosacea.
Q15: Why is my rosacea so red and inflamed?
The redness and inflammation of rosacea — including vascular dilation, flushing, and persistent erythema — are the skin’s visible expression of mast cell activation and the downstream inflammatory cascade it produces. In Demodex-driven rosacea, the mites and their waste products trigger a delayed hypersensitivity response from Langerhans cells that have lost their normal tolerance to Demodex. This immune reaction amplifies mast cell activation, increases histamine release, and drives the vascular reactivity that produces characteristic redness. Additionally, ATP released from dying Demodex cells acts as a danger signal that further amplifies the inflammatory response — a mechanism that explains why Demodex-driven rosacea can produce such intense and persistent redness even with relatively modest mite counts. The inflammation is not disproportionate — it is the immune system responding to a commensal it has been dysregulated into treating as a threat.
Written by Natalie Maibenko – a Certified Functional Medicine Practitioner and Master Esthetician with 22+ years of experience and founder of Unique Verve

As a Certified Functional Medicine Practitioner my Expertise Encompasses:
- Immune System: frequent illness, UTIs, yeast infections
- Allergies, Asthma
- Skin Problems: acne, cystic acne, rosacea, eczema, dermatitis, ichthyosis, psoriasis, vitiligo, melasma
- Inflammation: arthritis, rhinitis, joint & muscle pain, migraines, headaches
- Sleep Disturbunces, Insomnia
- Gut Problems: IBS/IBD, bloating, acid reflux, gas, constipation, diarrhea, parasites, fungal/yeast overgrowths
- Hormonal Imbalances: PCOS, PMS symptoms, weight problems/inability to lose weight, thyroid problems
- Hair Loss, Alopecia
- Mood Imbalances: anxiety, depression, irritability
- Metabolic Dysfunction, Insulin Resistance, Type 2 Diabetes
- Optimizing Wellness for Successful Pregnancy
- Autoimmune Conditions: Hashimoto’s thyroiditis, grave’s disease, reumatoid arthritis (RA), lupus, etc
- Bone Health: osteopenia/ osteoporosis
- Effective Anti-Aging Strategies without Injectables with the inside-out & outside-in approach
- Detoxification of Heavy Metals, Mycotoxins, Environmental Toxins
- Reversing Breast Implant Illness
- Preparation for the Explant Surgery and Optimization of Wellness & Vitality Post-Explant
With love and gratitude,
Natalie Maibenko
Functional Medicine & Skincare Expert – Helping You Take Control of Your Health and Achieve Lasting Skin Results Nationwide — Virtual Practice