Introduction
H. Pylori SIBO rosacea connection — three clinical entities that conventional dermatology almost never investigates together, yet that co-occur with striking consistency in women with treatment-resistant rosacea, and that share a common upstream environment: a weakened immune system, impaired thyroid function, and dysregulated blood sugar that together create the conditions in which these infections take hold, persist, and drive systemic inflammatory disease that expresses itself on the face.
Rosacea is not a skin condition with some gut triggers. It is a systemic, immune-blood sugar-thyroid mediated inflammatory disease that shows up on the skin. That reframing matters — because it changes everything about how the condition needs to be investigated and addressed.
In my functional medicine and functional dermatology practice, I consistently find H. Pylori infection and small intestinal bacterial overgrowth (SIBO) as active drivers in rosacea patients who have not responded to conventional treatment. What makes this pattern clinically important is not just the presence of the infections — it is understanding why the immune system is unable to keep them in check, and why antibiotics not only fail to resolve the root cause but frequently worsen the internal environment over time.
H. Pylori is endemic — it is present in a significant portion of the global population. SIBO is a translocation event — bacteria migrating where they should not be. A well-primed, appropriately balanced immune system is capable of maintaining equilibrium in the gut. The question I always ask is not how to eradicate the infection, but why the immune system lost its ability to keep peace in the first place. That upstream investigation is where lasting resolution begins.
This post breaks down the full clinical picture: how H. Pylori and SIBO drive rosacea through interconnected mechanisms, the upstream environment of thyroid dysfunction, blood sugar dysregulation, and chronic stress that allows them to thrive, why conventional antibiotic treatment perpetuates rather than resolves the cycle, and what a root-cause functional medicine approach actually looks like. As always, every protocol I build is individualized to what your specific testing reveals — what follows is the clinical framework I work within.
H. Pylori SIBO Rosacea: A Systemic Disease Beyond the Skin
The conventional dermatology model treats rosacea as a skin condition — one with internal triggers, perhaps, but fundamentally a dermatological problem requiring dermatological management. This framing is the source of most treatment failure.
A growing body of research confirms what functional medicine has long observed clinically: rosacea is a systemic, immune-mediated inflammatory disease. Published research has established significantly higher prevalence of gastrointestinal disorders and autoimmune risk — including SIBO, H. Pylori infection, celiac disease, Crohn’s disease, ulcerative colitis, and IBS — in rosacea patients compared to the general population. This is not coincidence. It is evidence of a shared upstream inflammatory environment in which gut infections and skin inflammation are parallel expressions of the same systemic dysfunction.
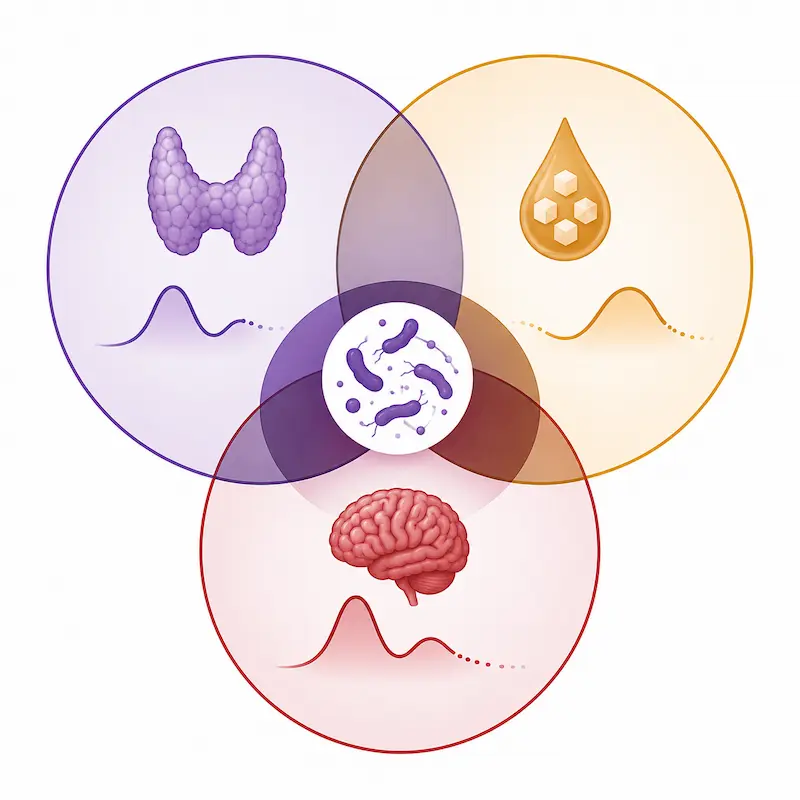
In my clinical experience, the most accurate framing is even more specific: rosacea is an immune-blood sugar-thyroid mediated systemic inflammatory disease. These three systems — immune function, glycemic regulation, and thyroid health — form the upstream environment that either maintains gut equilibrium or creates the conditions for H. Pylori and SIBO to thrive, persist, and drive the cascade that ultimately manifests as facial inflammation.
Understanding this is not just academically important. It is practically essential — because it explains why topical antibiotics quiet the skin temporarily, why oral antibiotics fail to produce lasting results, and why the same infections recur. None of these treatments address the upstream environment. The infections come back because the conditions that allowed them to take hold in the first place have not changed.
The Upstream Environment: Why H. Pylori and SIBO Take Hold
Before addressing what H. Pylori and SIBO do to the gut and the skin, it is essential to understand what allows them to thrive in the first place. Three interconnected upstream drivers create the internal environment in which these infections establish themselves and resist clearance.
1. Thyroid Dysfunction: The Gateway to Gut Overgrowth
Low thyroid function is one of the most clinically significant and most frequently overlooked upstream drivers of both H. Pylori persistence and SIBO development — and it is particularly prevalent in women, especially during the perimenopausal transition.
The thyroid governs metabolic rate across every organ system. In the gut, suboptimal thyroid function reduces the production of stomach acid, digestive enzymes, and bile — the primary chemical defenses against microbial overgrowth in the upper GI tract. Reduced stomach acid creates an environment in which H. Pylori can establish and maintain colonization more easily, and in which bacteria that should be killed before reaching the small intestine survive to proliferate there — the defining mechanism of SIBO.
Beyond its digestive effects, thyroid dysfunction directly impairs immune function. A sluggish thyroid reduces the activity of immune cells responsible for pathogen clearance — including the mucosal immune defenses that are the gut’s first line of response to bacterial overgrowth. This is a critical and frequently missed clinical connection: the immune system’s inability to clear H. Pylori and contain bacterial translocation in SIBO is not always a primary immune failure. It is often a downstream consequence of suboptimal thyroid function reducing immune competence.
Nutrient insufficiencies compound this further. Thyroid dysfunction impairs the absorption of the very nutrients required for immune function — zinc, selenium, iron, vitamin D, and amino acids. As nutrient status declines, immune competence declines further, creating a progressive weakening of the gut’s defense capacity that allows both H. Pylori and SIBO to consolidate.
Through a functional medicine lens, a TSH above 2 warrants full thyroid panel investigation — including free T3, free T4, reverse T3, and both antibodies. Suboptimal thyroid function that falls within conventional normal ranges can be a significant upstream driver of the entire gut infection picture and must not be overlooked because a single TSH value appears acceptable.
2. Blood Sugar Dysregulation and Insulin Resistance
Chronically elevated blood sugar creates a profoundly hospitable environment for bacterial overgrowth. Glucose is a direct substrate for pathogenic bacteria — elevated blood sugar feeds H. Pylori and SIBO simultaneously, sustaining their populations regardless of other interventions. This is one of the most underappreciated reasons why gut infections are so difficult to clear in patients with insulin resistance or metabolic dysfunction.
Beyond feeding the infections directly, insulin resistance and high blood sugar impair immune function through multiple mechanisms: reducing neutrophil and macrophage activity, impairing the secretory IgA response in the gut mucosa, and promoting the systemic inflammation that shifts immune resources away from pathogen surveillance. A body managing chronic metabolic inflammation has fewer immunological resources available for bacterial clearance.
Elevated blood sugar also damages tissues directly through glycation — including the acid mantle of the skin, impairing its barrier function and increasing vascular reactivity. Just as leaky gut allows bacterial fragments into circulation, a compromised acid mantle reduces the skin’s first line of defense against external triggers, amplifying the reactivity that drives rosacea flares. The connection between blood sugar, barrier compromise, and rosacea is not metaphorical — it is a direct tissue-level consequence of chronic glycation.
During the perimenopausal transition, declining estrogen and progesterone directly worsen insulin sensitivity, creating a compounding interaction: perimenopause drives insulin resistance, insulin resistance feeds bacterial overgrowth, bacterial overgrowth drives gut inflammation and systemic immune dysregulation, and the skin expresses the result.
3. Chronic Stress and MMC Dysfunction
Chronic stress impairs gut health through multiple mechanisms — elevating cortisol, increasing intestinal permeability, depleting secretory IgA, and suppressing the mucosal immune response. But the most direct and most frequently overlooked stress-gut connection in the context of SIBO is its effect on the migrating motor complex (MMC).
The MMC is the gut’s housekeeping mechanism — a series of electrical waves that sweep through the small intestine between meals, clearing residual bacteria and food particles and preventing their accumulation. When the MMC functions properly, bacterial populations in the small intestine are kept in check through this regular mechanical clearance. When it is impaired, bacteria accumulate between meals and SIBO develops or recurs.
Chronic stress directly suppresses MMC activity by dysregulating the enteric nervous system and reducing the motilin signaling that initiates the MMC sweep. Hypothyroidism compounds this — slowed gut motility from suboptimal thyroid function reduces MMC frequency and amplitude simultaneously. Together, stress and thyroid dysfunction impair the gut’s primary mechanical defense against bacterial overgrowth, creating conditions in which SIBO develops, persists, and recurs regardless of antimicrobial treatment — because the underlying motility dysfunction has not been addressed.
How H. Pylori Drives Rosacea: The Four-Part Cascade
H. Pylori is a gram-negative bacterium that colonizes the gastric mucosa and has evolved sophisticated mechanisms for evading immune clearance. In the context of rosacea, its effects operate through four interconnected pathways that collectively produce the systemic inflammatory environment driving skin inflammation.
1. Gastric Acid Suppression and the SIBO Gateway
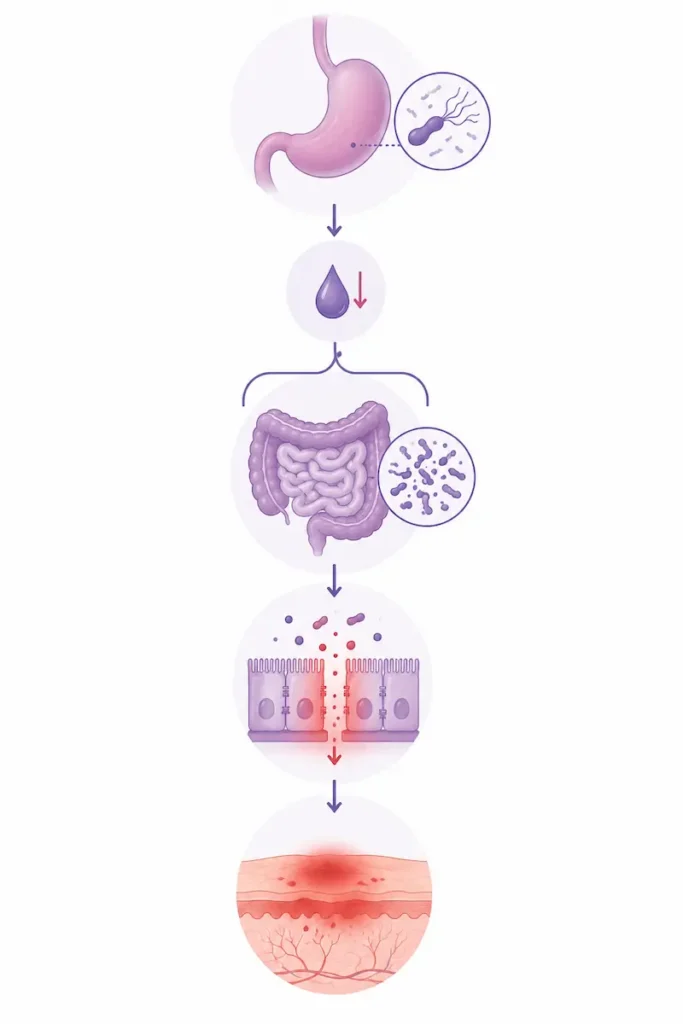
H. Pylori produces urease — an enzyme that converts urea into ammonia, raising the pH of the local gastric environment and effectively neutralizing stomach acid. This is the bacterium’s primary survival mechanism: by reducing gastric acidity, it protects itself from the acid that would otherwise clear it.
The downstream consequence is significant. Reduced stomach acid does not just protect H. Pylori — it creates a permissive environment throughout the upper GI tract. Bacteria that would normally be killed by gastric acid before reaching the small intestine now survive and migrate there. This is the direct gateway from H. Pylori infection to SIBO development. The two conditions are not coincidental co-occurrences — H. Pylori actively creates the conditions in which SIBO thrives.
2. Direct Immune Stimulation and Pro-Inflammatory Cytokine Release
H. Pylori is a potent immune stimulant. Its cell wall components — including lipopolysaccharides and outer membrane proteins — activate the innate immune system, triggering the release of pro-inflammatory cytokines including TNF-alpha, IL-1, IL-6, and IL-8. This systemic cytokine release does not remain localized to the stomach. It enters circulation and drives systemic inflammation — including the mast cell activation, vascular reactivity, and skin inflammation characteristic of rosacea.
H. Pylori also stimulates gastrin production — a hormone that in turn stimulates histamine release from enterochromaffin-like cells in the gastric mucosa. This gastrin-histamine pathway directly connects H. Pylori infection to histamine excess — the same histamine overload driving mast cell activation and vascular reactivity in rosacea. For patients with rosacea and H. Pylori, the histamine bucket is being filled from a source that no elimination diet or antihistamine can address without clearing the infection.
3. Gut Lining Damage and Nutrient Malabsorption
Chronic H. Pylori infection damages the gastric mucosa directly — impairing the production of intrinsic factor required for B12 absorption, reducing the absorption of iron, zinc, and amino acids, and creating the conditions for increased intestinal permeability. This nutrient malabsorption has cascading consequences: B12 deficiency impairs methylation and systemic histamine breakdown; zinc deficiency impairs immune function and skin barrier integrity; amino acid insufficiency reduces the production of stomach acid, digestive enzymes, and the structural proteins needed for gut lining repair.
The malabsorption of amino acids deserves specific clinical attention. Amino acids are the building blocks of digestive enzymes, stomach acid components, neurotransmitters, and immune proteins. When H. Pylori impairs their absorption, it undermines virtually every downstream system simultaneously — perpetuating the thyroid-immune-digestive dysfunction that allowed it to establish in the first place.
4. DAO Impairment and Histamine Accumulation
The damage H. Pylori inflicts on the gut lining — combined with the dysbiosis and SIBO it facilitates — directly impairs DAO enzyme production. As we have explored in detail in our post on the histamine-rosacea gut connection, DAO is the primary enzyme responsible for breaking down histamine in the gut. When the intestinal lining is damaged, DAO production is reduced, histamine accumulates systemically, and mast cell activation amplifies the vascular reactivity and skin inflammation driving rosacea.
The H. Pylori-gastrin-histamine pathway and the gut lining-DAO pathway represent two parallel mechanisms through which a single infection drives histamine excess — and neither can be adequately addressed through antihistamines, elimination diets, or topical rosacea treatment without clearing the underlying infection and restoring gut integrity.
How SIBO Drives Rosacea: Hydrogen vs. Methane and Why It Matters
Small intestinal bacterial overgrowth occurs when bacteria that normally populate the large intestine migrate into and colonize the small intestine — where they do not belong and where their presence creates significant local and systemic consequences. Understanding SIBO requires distinguishing it from general gut dysbiosis, and understanding that there are two primary types of SIBO that produce distinctly different symptom pictures.
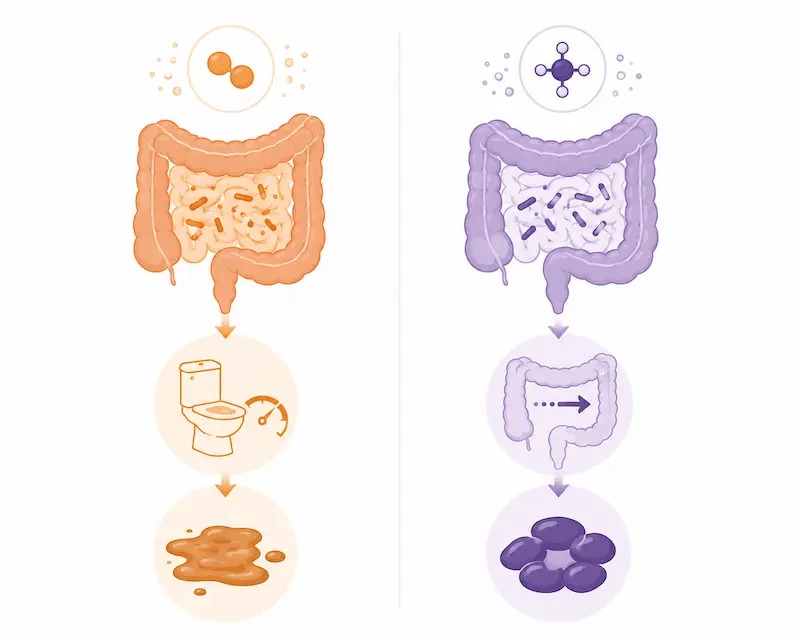
Hydrogen-Dominant SIBO
Hydrogen-dominant SIBO occurs when bacteria in the small intestine ferment carbohydrates and produce primarily hydrogen gas. The symptoms are typically: bloating that worsens after meals, abdominal distension, flatulence, and loose stools or diarrhea. The hydrogen-producing bacteria accelerate intestinal transit, which is why loose stool patterns are the hallmark presentation. Readers who recognize the pattern of bloating after eating followed by urgency and loose stool are describing the hydrogen SIBO picture.
Methane-Dominant SIBO (Intestinal Methanogen Overgrowth)
Methane-dominant SIBO — more accurately called intestinal methanogen overgrowth (IMO) — involves archaea rather than bacteria, producing methane gas through fermentation. Methane has a direct inhibitory effect on intestinal motility — it slows transit time, producing the opposite symptom picture from hydrogen SIBO: constipation, bloating that persists throughout the day rather than peaking after meals, and a feeling of fullness or sluggishness. Women who have been told they have IBS with constipation, who have tried multiple dietary interventions without relief, and who also have rosacea, are frequently presenting with methane-dominant SIBO as an unidentified component of their picture.
The distinction matters clinically because the two types respond differently to interventions — both botanical and pharmaceutical. Testing with a lactulose or glucose breath test, or through comprehensive stool analysis, identifies which type is present and informs the appropriate protocol.
How SIBO Drives Rosacea Systemically
Regardless of type, SIBO drives rosacea through the same core mechanisms: bacterial fermentation produces endotoxins and LPS that translocate through a compromised intestinal barrier into circulation, activating mast cells systemically and driving the cytokine release that produces facial inflammation. The brush border damage caused by bacterial overgrowth in the small intestine directly impairs nutrient absorption — compounding the malabsorption already initiated by H. Pylori and reducing the nutrient cofactors needed for DAO enzyme function, histamine breakdown, and immune competence.
SIBO also drives intestinal permeability directly. The overgrowth of bacteria in the small intestine produces organic acids and other metabolites that damage tight junctions between epithelial cells — creating or worsening leaky gut and amplifying LPS translocation into circulation. For patients who have been told their rosacea is “just a skin condition,” the presence of SIBO means their small intestine is actively producing and releasing bacterial fragments into their bloodstream that their immune system is responding to in the skin.
Why Antibiotics Keep Failing — And Making Things Worse
The conventional treatment for H. Pylori is triple or quadruple antibiotic therapy — typically combining two or three antibiotics with a proton pump inhibitor (PPI). The conventional treatment for SIBO is rifaximin, sometimes combined with neomycin for methane-dominant presentations. Both approaches share a fundamental limitation: they target the infection without addressing the upstream environment that allowed it to develop and that will allow it to return.
Beyond this limitation, antibiotic treatment for gut infections creates specific downstream consequences that worsen the internal environment and gut health:
- Microbiome devastation — broad-spectrum antibiotics eliminate beneficial bacteria alongside pathogenic ones, reducing microbial diversity, impairing the estrobolome, reducing DAO-producing bacterial populations, and creating the dysbiotic environment in which both H. Pylori and SIBO recurrence is more likely, not less.
- Gut lining compromise — antibiotics impair the integrity of the intestinal epithelium, worsening leaky gut, increasing LPS translocation, and reducing the barrier function that is already compromised in these patients.
- Nutrient depletion — antibiotics deplete B vitamins, vitamin K, and minerals that are essential for thyroid function, immune competence, DAO enzyme production, and histamine breakdown — weakening the very systems needed to prevent recurrence.
- Antibiotic resistance — H. Pylori eradication rates with standard triple therapy have declined significantly as antibiotic resistance has increased. In many cases, the full antibiotic course fails to clear the infection entirely, leaving resistant strains that are harder to address on subsequent attempts.
- PPI consequences — proton pump inhibitors used alongside H. Pylori antibiotic therapy further reduce stomach acid, directly worsening the gastric environment that feeds SIBO and impairs nutrient absorption long after the antibiotic course ends.
The recurrence pattern that many patients experience — treating H. Pylori or SIBO with antibiotics, seeing temporary improvement, and then watching the infections return — is a predictable consequence of this approach. The upstream environment has not changed. The immune system has been further weakened. The gut lining has been further compromised. The conditions for recurrence are, in many cases, better after antibiotic treatment than before it.
A Patient Story: When the Gut Was Telling the Whole Story
One of my patients came to me primarily to address her gut issues — she had not connected her rosacea to the rest of what was happening in her body, and she was not seeking skin treatment. She had been managing her rosacea separately with conventional treatment for years.
Her symptom picture was extensive: daily bloating, IBS symptoms with loose stool patterns occurring two to three times weekly, poor sleep with frequent waking in the middle of the night and difficulty returning to sleep, blurry vision, hoarse voice, mood imbalances including bursts of anger, crying episodes, and depression, severe PMS with breast tenderness, hair loss, and joint pain. Her nails showed ridges and white dots — visible evidence of the nutrient insufficiencies that chronic gut dysfunction had produced over time.
Her Gut Zoomer revealed elevated SIBO markers alongside significant dysbiosis. The nutrient malabsorption driven by chronic SIBO had depleted the cofactors needed for thyroid function, immune competence, and neurotransmitter synthesis — which explained the sleep disruption, mood imbalances, hair loss, joint pain, and the visual and vocal symptoms that she had been attributing to aging and stress.
What she had not connected — and what her conventional practitioners had not identified — was that her rosacea was one of many downstream expressions of the same upstream dysfunction. The same gut-driven systemic inflammation producing her daily bloating and loose stools was also producing her facial redness and reactivity. The same nutrient insufficiency impairing her thyroid and immune function was also impairing the DAO enzyme production that would have broken down the histamine driving her skin flares.
Her protocol addressed the full picture systematically — gut restoration, SIBO clearance, thyroid and immune support, targeted nutrient repletion, and motility support with Mag+Malic and 5-HTP Plus. After three months on the functional medicine program, she was free of all symptoms. Her digestion normalized. Her sleep consolidated. Her mood stabilized. Her hair loss stopped and regrowth began. Her joint pain resolved. Her vision improved. And her rosacea cleared significantly — not because we treated her skin, but because we addressed what her skin had been signaling all along.
The Most Important Thing to Understand About H. Pylori SIBO Rosacea Connection
H. Pylori is endemic. SIBO is translocation. A well-primed, appropriately balanced immune system is capable of maintaining peace in the gut. The question is never just how to eradicate the infection — it is why the immune system lost its ability to keep it in check.
Antibiotics cannot answer that question. They can temporarily reduce the bacterial load — though increasingly less effectively as resistance grows — but they cannot restore thyroid function, rebuild immune competence, correct nutrient insufficiencies, repair gut motility, restore MMC activity, or rebuild the intestinal barrier. And because they decimate the microbiome while doing so, they frequently leave the patient with a weaker immune system, a more compromised gut, and a higher likelihood of recurrence than before treatment.
The functional medicine approach to H. Pylori, SIBO, and rosacea does not start with the infections. It starts with the upstream environment — the thyroid dysfunction, blood sugar dysregulation, chronic stress, and nutrient insufficiencies that created the conditions in which the infections could establish and the immune system lost its capacity to contain them. Address those root causes, and the body regains the competence it needs to clear and prevent recurrence of the infections that are driving the skin.
Your rosacea is not a skin problem that happens to have some gut triggers. It is a systemic signal from a body asking for upstream investigation. The infections are part of the message. The message is that something further upstream needs to change.
This is the foundation of my functional medicine and functional dermatology practice. The skin is the signal. The work is internal.
I offer virtual Initial Functional Medicine Health and Skin Assessments for anyone who is ready to look upstream. This is where we take a full picture of your health history, your current symptoms, and the patterns that connect them — and build a testing and protocol strategy specific to your body.
→ Book your Initial Functional Medicine Health and Skin Assessment
Frequently Asked Questions
Q1: Does my gut health cause my rosacea?
In a significant subset of rosacea patients, gut infections and dysbiosis are central drivers of the facial inflammation — not peripheral triggers. H. Pylori infection and SIBO both drive rosacea through multiple mechanisms: direct immune system stimulation producing pro-inflammatory cytokines that drive mast cell activation in the skin, gut lining damage impairing DAO enzyme production and allowing histamine accumulation, LPS translocation from a leaky gut into circulation, and nutrient malabsorption depleting the cofactors needed for histamine breakdown and immune regulation. For these patients, rosacea will not clear meaningfully until the gut infections are identified and addressed.
Q2: Can fixing my gut reduce rosacea flare-ups?
Yes — often significantly. When H. Pylori, SIBO, or gut dysbiosis are the primary drivers of rosacea, addressing them systematically produces improvements in skin reactivity, redness, and flushing that topical treatment and trigger avoidance cannot achieve alone. The key is identifying which specific gut infections and imbalances are present through comprehensive testing, and addressing the upstream environment — thyroid function, immune competence, blood sugar regulation — that allowed them to develop. Gut restoration without addressing the upstream environment frequently produces incomplete or temporary results.
Q3: What gut problems trigger rosacea flares?
The gut conditions most consistently associated with rosacea include H. Pylori infection, small intestinal bacterial overgrowth (SIBO), leaky gut (increased intestinal permeability), and general dysbiosis. Each drives rosacea through distinct mechanisms — H. Pylori through gastrin-histamine stimulation and direct cytokine release, SIBO through bacterial fermentation producing endotoxins that enter circulation through a compromised intestinal barrier, leaky gut through LPS translocation activating mast cells systemically. In many patients, more than one of these is present simultaneously — because the upstream environment of thyroid dysfunction, blood sugar dysregulation, and chronic stress creates the conditions for all of them to develop together.
Q4: Is my rosacea actually a gut problem?
It may be a central part of the picture — and it is almost never investigated in conventional dermatology. Rosacea is a systemic immune-mediated inflammatory disease, not just a skin condition. For patients with digestive symptoms alongside their rosacea — bloating, IBS symptoms, acid reflux, constipation, loose stool patterns — the gut connection is highly likely and warrants comprehensive functional medicine testing. The fact that you have rosacea and digestive symptoms that you consider unrelated is, clinically, one of the most important signals that they share a common upstream cause.
Q5: How to tell if gut dysbiosis is causing my rosacea?
The most reliable way is comprehensive functional medicine testing — specifically the Gut Zoomer, which assesses microbiome composition, detects H. Pylori and SIBO markers, measures inflammatory markers, and evaluates intestinal permeability alongside digestive function. Clinically, the combination of rosacea with digestive symptoms (bloating, IBS patterns, acid reflux), systemic symptoms (joint pain, brain fog, mood imbalances), and a history of antibiotic use or conventional rosacea treatment that has not produced lasting results is a strong pattern suggesting gut dysbiosis as a central driver. Testing confirms what the symptom picture suggests.
Q6: Why did my rosacea get worse after antibiotics?
Because antibiotics address the visible infection without addressing the upstream environment that allowed it to develop — and they create significant downstream consequences in the process. Antibiotics decimate the gut microbiome, reducing the beneficial bacterial populations responsible for histamine breakdown, immune regulation, and intestinal barrier integrity. They deplete B vitamins and minerals needed for thyroid function and immune competence. They worsen gut lining damage and increase intestinal permeability. When the antibiotic course ends, the internal environment is frequently more compromised than before — the immune system is weaker, the microbiome is less diverse, and the conditions for recurrence and worsening skin reactivity are better, not worse.
Q7: Can probiotics help rosacea?
Yes — but strain selection matters significantly, and not all probiotics are appropriate in rosacea cases with a histamine component. Certain bacterial strains produce histamine, which can worsen mast cell activation and skin reactivity. Clinically, I use Probiotic Integrum — a formulation selected specifically for its histamine-conscious strain profile — as part of the gut restoration protocol. Probiotics are most effective as part of a comprehensive protocol that also addresses the infections, gut lining damage, and upstream immune and thyroid dysfunction driving the dysbiosis. As a standalone intervention, probiotics rarely produce significant or lasting rosacea improvement.
Q8: Why does my rosacea keep coming back?
Recurrent rosacea — particularly after antibiotic courses that provided temporary improvement — almost always indicates that the upstream drivers have not been identified or addressed. H. Pylori and SIBO recur when the internal environment that allowed them to develop — suboptimal thyroid function, impaired MMC motility, blood sugar dysregulation, depleted immune competence — remains unchanged. The infection comes back because the immune system is still unable to maintain balance in the gut. Lasting resolution requires correcting the upstream environment, not repeating the antibiotic course.
Q9: Should I get tested for SIBO before treating my skin?
If you have rosacea, hormonal acne, or eczema that has not responded meaningfully to conventional treatment — and particularly if you have any digestive symptoms running alongside your skin condition — yes, SIBO testing should be part of a comprehensive functional medicine workup. The reason is clinical efficiency: treating skin inflammation without identifying whether SIBO is an active driver means treating the downstream expression while leaving the upstream source intact. SIBO damages the gut lining through bacterial fermentation and organic acid production — and it is this intestinal lining damage that creates the permeability allowing bacterial endotoxins to translocate into circulation and activate the mast cell-histamine cascade driving skin inflammation. The skin may improve temporarily with topical treatment, but as long as SIBO is actively damaging the gut lining and sustaining that permeability, the internal environment producing the skin condition remains intact. Identifying SIBO through the Gut Zoomer allows the protocol to target the actual driver rather than cycling through symptomatic management.
Written by Natalie Maibenko – a Certified Functional Medicine Practitioner and Master Esthetician with 22+ years of experience and founder of Unique Verve

As a Certified Functional Medicine Practitioner my Expertise Encompasses:
- Immune System: frequent illness, UTIs, yeast infections
- Allergies, Asthma
- Skin Problems: acne, cystic acne, rosacea, eczema, dermatitis, ichthyosis, psoriasis, vitiligo, melasma
- Inflammation: arthritis, rhinitis, joint & muscle pain, migraines, headaches
- Sleep Disturbunces, Insomnia
- Gut Problems: IBS/IBD, bloating, acid reflux, gas, constipation, diarrhea, parasites, fungal/yeast overgrowths
- Hormonal Imbalances: PCOS, PMS symptoms, weight problems/inability to lose weight, thyroid problems
- Hair Loss, Alopecia
- Mood Imbalances: anxiety, depression, irritability
- Metabolic Dysfunction, Insulin Resistance, Type 2 Diabetes
- Optimizing Wellness for Successful Pregnancy
- Autoimmune Conditions: Hashimoto’s thyroiditis, grave’s disease, reumatoid arthritis (RA), lupus, etc
- Bone Health: osteopenia/ osteoporosis
- Effective Anti-Aging Strategies without Injectables with the inside-out & outside-in approach
- Detoxification of Heavy Metals, Mycotoxins, Environmental Toxins
- Reversing Breast Implant Illness
- Preparation for the Explant Surgery and Optimization of Wellness & Vitality Post-Explant
With love and gratitude,
Natalie Maibenko
Functional Medicine & Skincare Expert – Helping You Take Control of Your Health and Achieve Lasting Skin Results Nationwide — Virtual Practice
Disclaimer: Information and content on this website is provided for educational purposes only, and is not intended to diagnose, treat and to be a substitute for the advice provided by your physician or other healthcare professional. No information offered here should be interpreted as a diagnosis of any disease, nor an attempt to treat or prevent or cure any disease or condition. If you have any concerns or questions about your health, you should always consult with a physician or other healthcare professional. Do not disregard, avoid, or delay obtaining medical or health-related advice from your healthcare professional. Always speak with your healthcare professional before taking any medications, supplements or pursuing any wellness programs. Information provided on this website does not create a doctor-patient relationship between you and any professional affiliated with this website.