Introduction
Signs and symptoms of histamine intolerance are among the most consistently missed patterns in conventional medicine — not because the symptoms are subtle, but because they are so widespread across so many organ systems simultaneously that no single specialist is positioned to connect them. The cardiologist investigates the palpitations. The dermatologist manages the urticaria, eczema and rosacea. The gastroenterologist works on the IBS picture. The psychiatrist addresses the anxiety and depression. And nobody — in any of those appointments — asks the question that ties all of it together: is histamine overload the common upstream driver of everything you are experiencing?
In my functional medicine practice, I see histamine intolerance as one of the most under-recognized and over-complicated conditions affecting women in their 30s, 40s, and beyond. The reason it falls through the diagnostic cracks is both structural and conceptual. Structurally, conventional medicine has no official disease label for histamine intolerance or histamine overload — and without a label, there is no billing code, no standard treatment protocol, and no specialist whose remit it falls within. Conceptually, conventional medicine treats each organ system in isolation, while histamine — a potent immune mediator produced throughout the body in response to inflammation — operates systemically, crossing every organ system simultaneously.

Functional medicine approaches this differently. Rather than requiring a disease label to validate a symptom, functional medicine looks at symptom patterns, the interconnectedness of systems, and the upstream drivers that produce the pattern. Histamine intolerance is not a disease in the conventional sense. It is a state of histamine excess relative to the body’s capacity to break it down — a state with specific, identifiable, and addressable upstream causes that conventional medicine is not structured to investigate.
This post covers the full spectrum of signs and symptoms of histamine intolerance, why they appear across so many systems simultaneously, and what the upstream picture looks like. If you have been dismissed, given a diagnosis that explains only part of your symptom picture, or told your results are normal while you continue to feel anything but — this post is written for you. As always, every protocol is individualized to what your specific testing, health history and collective symptom patterns reveal.
What Is Histamine Intolerance — And Why Doesn’t Conventional Medicine Recognize It?
Understanding what produces the signs and symptoms of histamine intolerance begins with understanding what histamine actually is and what happens when it accumulates beyond the body’s capacity to degrade it.
Histamine is a biogenic amine produced throughout the body by mast cells, basophils, enterochromaffin cells, and histaminergic neurons. It serves essential biological functions: it is a key mediator of the immune response, a regulator of gastric acid secretion, a neurotransmitter in the brain, and a signaling molecule in the gut. Under healthy conditions, histamine is produced, acts on its target receptors, and is then rapidly degraded by two primary enzymes: diamine oxidase (DAO) in the gut and N-methyltransferase (HNMT) intracellularly and in tissues. HNMT can be impaired by MTHFR, MTR and MTRR SNPs (genetic impairments).
Histamine intolerance occurs when histamine accumulates faster than the body can degrade it — creating a systemic excess that activates histamine receptors throughout the body and produces the broad, multi-system symptom picture that makes this condition so difficult to identify through a conventional diagnostic lens.
The reason histamine intolerance has no conventional disease label is both practical and philosophical. Practically, DAO enzyme activity is not measured in standard blood panels, and histamine blood levels fluctuate too rapidly to be reliably captured in a single draw. Without a direct, standardized, reproducible measurement, conventional medicine has no objective marker to attach a diagnosis to. Philosophically, the conventional model requires symptoms to map onto a specific organ or system to be assigned to a specialty — and histamine intolerance maps onto every system simultaneously, which means it belongs to no specialty and therefore to none.
Functional medicine does not require a disease label to recognize and address a pattern. The signs and symptoms of histamine intolerance, the clinical history, the upstream drivers revealed through targeted testing, and the response to interventions that reduce histamine load and restore degradation capacity together constitute a clear and actionable clinical picture — one that resolves when addressed correctly and worsens when ignored.
Signs and Symptoms of Histamine Intolerance: The Full Multi-System Picture
The breadth of the signs and symptoms of histamine intolerance is both its most clinically important feature and the primary reason it goes unrecognized. A patient who presents with urticaria and anxiety will be seen by a dermatologist and a psychiatrist on separate occasions, each treating their respective symptom without awareness of the shared upstream driver. Understanding the full spectrum — and the mechanism connecting each symptom to histamine excess — is the starting point for pattern recognition.
Skin
Among the signs and symptoms of histamine intolerance, the skin picture is often the most visible — and the most likely to be treated in isolation by a dermatologist who never asks about the gut, mood, or cardiovascular symptoms present simultaneously. Signs and symptoms of histamine intolerance in the skin include urticaria (hives), pruritus (itching), flushing and redness, rosacea, eczema, acne, and general skin reactivity — skin that reacts to products, temperatures, and environmental exposures it previously tolerated without response.
The mast cell activation driving these skin symptoms is identical to the mechanism driving rosacea and eczema in the context of gut-skin axis dysfunction. For patients with skin conditions that have not responded to topical treatment, histamine overload is almost always part of the upstream picture that needs investigation.
Gut and Digestive System
The gastrointestinal tract is the primary site of both histamine production and histamine degradation. When DAO production is impaired — through gut lining damage, gut dysbiosis, nutrient insufficiency, or parasitic infection — histamine that should be degraded before reaching circulation accumulates in the gut and systemically. Gut signs and symptoms of histamine intolerance include bloating, gas, belching, burping, nausea, stomach pain and cramping, diarrhea, and loose stools. The gut irritability produced by histamine excess is frequently diagnosed as IBS — a label that describes the symptom pattern without investigating the histamine overload that may be producing it.
Neurological and Mood
Histamine is a significant neurotransmitter in the brain and central nervous system. When histamine crosses the blood-brain barrier — which it does more readily when gut permeability is increased and LPS translocation amplifies systemic immune activation — it produces neuroinflammatory signaling that manifests as a broad range of neurological and mood symptoms. Signs and symptoms of histamine intolerance in the neurological and mood domain include brain fog, difficulty concentrating, headaches, chronic irritability and anger, emotional reactivity and mood instability, anxiety, depression, emotional numbness, restlessness, and insomnia. These symptoms are frequently treated as primary psychiatric conditions — anxiety disorder, depression, mood disorder — without investigation of the histamine-driven neuroinflammatory picture that may be producing or amplifying them.
Cardiovascular
Histamine directly affects vascular tone and cardiac function through H1 and H2 receptor activation. The neurological and mood signs and symptoms of histamine intolerance are among the most frequently misattributed to primary psychiatric conditions. H1 receptor activation in blood vessels produces vasodilation, increased vascular permeability, and the flushing and redness visible in skin. H2 receptor activation in the heart increases heart rate and the strength of cardiac contractions.
Signs and symptoms of histamine intolerance in the cardiovascular system include heart palpitations, elevated resting heart rate, arrhythmia, flushing, and a sensation of warmth or racing in the chest. These symptoms are frequently investigated by cardiologists through standard cardiac workups that return normal results — because the histamine-driven vascular reactivity producing them is not captured by standard cardiac assessment.
Respiratory and Sinus
Histamine is one of the primary mediators of the allergic respiratory response. Signs and symptoms of histamine intolerance in the respiratory and sinus system include nasal congestion, sneezing, chronic sinusitis symptoms, postnasal drip, and increased susceptibility to respiratory illness. These symptoms are frequently managed with anti-histamines — which suppress the downstream histamine response without addressing the upstream overproduction or impaired degradation driving it. Importantly, anti-histamines monopolize the same detoxification pathways needed to clear the toxins that prime the immune system for histamine hyperreactivity — creating a paradox in which the treatment impairs the body’s ability to address the root cause.
Hormonal and Reproductive
Estrogen and histamine have a bidirectional relationship that makes histamine intolerance particularly relevant for women across the hormonal lifespan. Estrogen directly stimulates mast cells to produce and release histamine — which means that during the luteal phase of the menstrual cycle (days 14-28), when estrogen is relatively higher, histamine production increases and the histamine bucket fills more rapidly. This is why many women with histamine intolerance experience cyclical worsening of symptoms in the second half of their cycle. Conversely, histamine stimulates estrogen production — creating a bidirectional amplification loop. Signs and symptoms in this domain include severe PMS, painful periods, breast tenderness, mood imbalances and a cyclical pattern of symptom worsening that correlates with the luteal phase.
The estrogen dominance driving this histamine amplification does not require elevated estrogen production to occur. More often, it reflects either poor metabolism and clearance of the body’s own endogenous estrogens through the liver’s detoxification pathways, or — perhaps even more frequently — an accumulated estrogenic burden from xenoestrogenic chemicals in the environment.
These exogenous compounds, found in plastics, personal care products, household chemicals, heavy metals, mycotoxins and countless other ubiquitous sources, exert estrogen-like effects on the body’s estrogen receptors regardless of what a hormone panel shows for circulating estrogen levels. A woman can have entirely ‘normal’ bloodwork for estrogen while carrying a significant estrogenic burden from these sources — compounding the mast cell stimulation and histamine production described above without any conventional lab finding to explain it.
Sensory and Other
Additional signs and symptoms of histamine intolerance include tinnitus and ear buzzing, blurry vision, vulnerability to ongoing illness and frequent infections, and a generalized sense of being reactive to everything — foods, environments, products, and stressors that were previously tolerated without response. This global reactivity is one of the most diagnostically significant patterns: when a patient describes becoming progressively more sensitive to an expanding range of triggers, it almost always reflects a histamine bucket that is chronically full, leaving the immune system in a state of permanent hypervigilance where the threshold for reaction is vanishingly low.
The Histamine Bucket: Why Your Reactions Feel Random and Unpredictable
One of the most disorienting aspects of the signs and symptoms of histamine intolerance is their apparent inconsistency — reactions that seem random, unpredictable, and disconnected from any single identifiable trigger. A food that caused no reaction last week produces significant symptoms today. A glass of wine that was tolerable in summer triggers palpitations in autumn. A stressful week at work produces symptoms that seem entirely unrelated to food. The histamine bucket concept explains why.
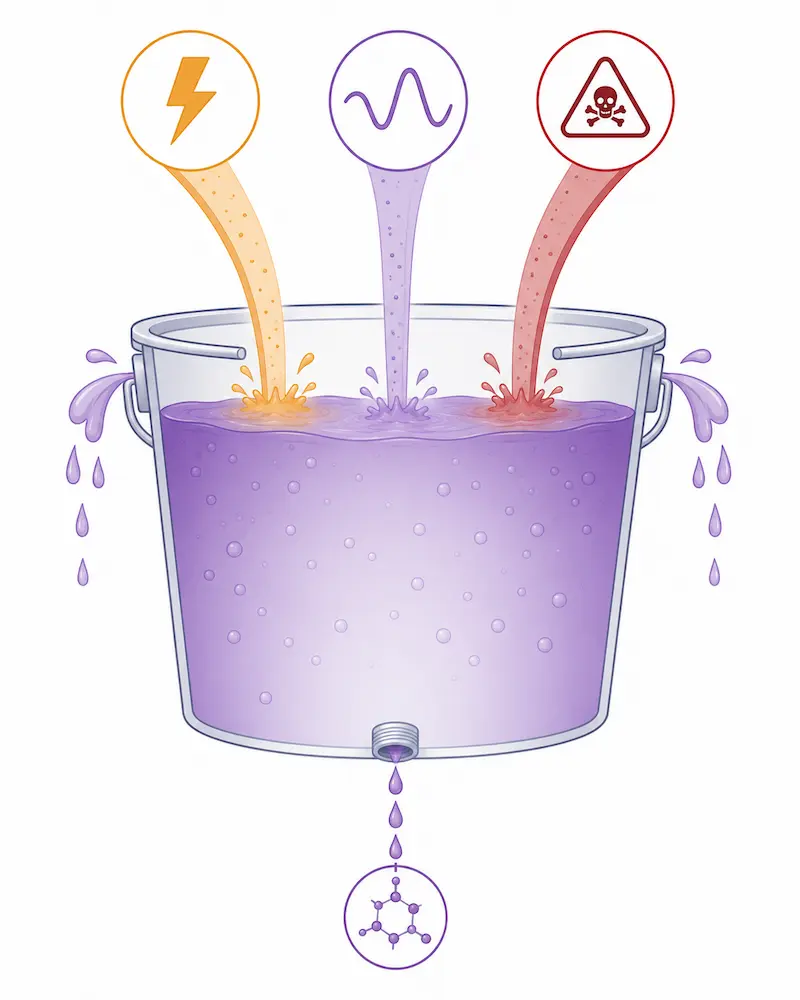
Think of your body’s histamine load as a bucket. Every source of histamine — high-histamine foods, gut bacteria producing histamine, mast cell activation from immune stimulation, estrogen-driven mast cell degranulation, environmental triggers, toxins, allergens — adds to the bucket. Every pathway that degrades histamine — DAO in the gut, HNMT in tissues, detoxification through the liver — drains the bucket. Symptoms occur not when a single trigger exceeds a fixed threshold, but when the cumulative load in the bucket overflows the body’s current degradation capacity.
The bucket fills differently on different days — and three dynamics compound each other with particular consistency in the women I see in my practice:
Stress depletes the nutrients required to degrade histamine — particularly vitamin B6 and vitamin C, which are essential DAO enzyme cofactors. A high-stress period does not just increase cortisol; it depletes the biochemical infrastructure needed to keep the histamine bucket draining. The same food eaten during a low-stress week and a high-stress week can produce entirely different responses because the bucket draining capacity is different.
Estrogen dominance — particularly during days 14-28 of the menstrual cycle when the luteal phase creates a relative estrogen elevation — directly stimulates mast cells to produce and release more histamine. For women approaching perimenopause, this dynamic can begin as early as age 35 as progesterone begins to decline relative to estrogen, removing its natural mast cell-stabilizing effect. The same hormonal shift that produces worsening PMS, mood instability, and cycle irregularity in perimenopause is simultaneously filling the histamine bucket more rapidly — which is why histamine intolerance symptoms so frequently worsen or first appear in the mid-to-late 30s and accelerate through perimenopause and beyond.
Toxin accumulation adds directly to the histamine bucket. When heavy metals, mycotoxins, and environmental chemicals are not biotransformed and cleared through the liver’s detoxification pathways in a timely manner, they prime the immune system for chronic hypervigilance — maintaining the mast cell activation that keeps histamine production elevated. Allergy season adds a further environmental histamine and immune activation load that compounds all three dynamics simultaneously. When stress, estrogen dominance, and toxin accumulation are all operating at once — which I see consistently in clinical practice — the histamine bucket overflows at exposures that would be completely tolerable in isolation.
What Creates the Histamine Overload: The Upstream Drivers
Histamine intolerance is never a primary condition. It is always downstream of upstream drivers that either increase histamine production beyond the body’s degradation capacity, impair the enzymatic machinery needed to degrade histamine, or both. In my practice, the following upstream drivers are the most consistently present — and they almost always compound each other.
Gut Dysbiosis, Leaky Gut, and Parasitic Infection
The gut lining is where DAO enzyme is produced — specifically in the brush border cells of the small intestinal epithelium. When the gut lining is damaged through dysbiosis, SIBO, parasitic infection, celiac or leaky gut, DAO production is reduced, histamine that should be degraded in the gut reaches circulation, and the inflammatory signals from a compromised gut lining activate mast cells systemically. Certain pathogenic gut bacteria also produce histamine directly as a metabolic byproduct, adding to the systemic load. Gut restoration is therefore not just supportive in histamine intolerance — it is foundational to restoring the degradation capacity the body needs to keep the histamine bucket draining.
Toxic Overload — The Most Overlooked Driver
Toxic overload — from heavy metals, environmental chemicals, and mycotoxins from mold exposure — is one of the most significant and most consistently overlooked upstream drivers of histamine intolerance. Toxins prime the immune system for chronic hypervigilance by maintaining a state of low-grade immune activation that keeps mast cells primed for degranulation. They also impair the liver’s biotransformation capacity — reducing its ability to process both toxins and histamine metabolites simultaneously.
The vicious cycle that toxic overload creates is clinically important to understand. Toxin exposure increases cortisol through HPA axis activation. Elevated cortisol increases thyroid hormone binding globulin (TBG), which binds free thyroid hormone and reduces its bioavailability — producing functional hypothyroidism even when TSH appears within the normal reference range. Low thyroid function then slows gut motility, reduces DAO production, impairs detoxification enzyme activity, and drives nutrient insufficiency. The resulting nutrient depletion further impairs DAO function and the liver’s capacity to biotransform toxins — creating a self-reinforcing cycle in which toxic overload, thyroid dysfunction, nutrient insufficiency, and histamine overload compound each other continuously.
If a patient is also taking antihistamines to manage symptoms, the cycle becomes even more entrenched. Antihistamines are metabolized through the same CYP450 detoxification pathways that the liver uses to biotransform toxins and endogenous as well as exogenous estrogens. By monopolizing these pathways, antihistamines reduce the liver’s capacity to clear the toxins driving the immune hypervigilance — making the root cause progressively harder to address while providing only partial and temporary symptom relief.
Hormonal Imbalance — Especially Estrogen Dominance
Estrogen directly stimulates mast cell degranulation and histamine release. In a state of estrogen dominance — whether from excess production, poor liver clearance, a disrupted estrobolome, or the progesterone decline of perimenopause — mast cells are more reactive, histamine production is amplified, and the capacity for histamine regulation is simultaneously reduced because progesterone’s mast cell-stabilizing effect has been removed. Hormonal contraception that uses synthetic progestins such as Mirena rather than bioidentical progesterone compounds this picture: synthetic progestins suppress the body’s natural progesterone production without providing its mast cell-stabilizing function, leaving the estrogenic mast cell stimulation unopposed.
Nutrient Insufficiencies Depleting DAO Cofactors
DAO enzyme requires vitamin B6, vitamin C, and copper as cofactors for its activity. When these nutrients are depleted — through chronic stress, poor absorption from gut dysbiosis or celiac, or high metabolic demand from ongoing immune activation — DAO enzyme activity is reduced regardless of how well the gut lining is otherwise functioning. B6 depletion is particularly relevant: chronic stress, oral contraceptive use, and poor gut absorption all deplete B6, and B6 deficiency impairs not only DAO activity but also the broader neurotransmitter synthesis that contributes to the mood and neurological symptoms of histamine intolerance.
Thyroid Dysfunction
Suboptimal thyroid function reduces gut motility, impairs DAO production, slows detoxification enzyme activity, and reduces immune competence — creating the internal environment in which histamine accumulates and the mechanisms needed to clear it are simultaneously impaired. The thyroid-histamine connection is bidirectional: toxic overload impairs thyroid function through TBG elevation, and thyroid dysfunction amplifies histamine overload through impaired DAO production and detoxification. This bidirectional loop is one of the most clinically important and most consistently overlooked dynamics in the histamine intolerance picture.
A Patient Case: When Everything Was Connected and Nothing Had Been Addressed
One of the most comprehensive histamine intolerance cases I have seen in my practice was a woman in early perimenopause — 39 years old — who came to me with a symptom picture that had been present in various forms since childhood and had escalated dramatically in her 30s.
Her presenting symptoms were extensive and spanned multiple systems: daily diarrhea occurring up to three times daily, severe gas, belching, and burping, severe stomach pain that she rated at the highest level of discomfort, severe PMS with painful periods, chronic and severe irritability and anger that was affecting her relationships and quality of life, mood instability, depression and emotional numbness, brain fog, restlessness, and daily headaches. She was using a Mirena hormonal IUD, which was suppressing her natural progesterone production through its synthetic progestin — removing the mast cell-stabilizing effect of progesterone and leaving estrogen’s mast cell-stimulating action unopposed. This was directly amplifying the estrogen-driven component of her histamine picture.
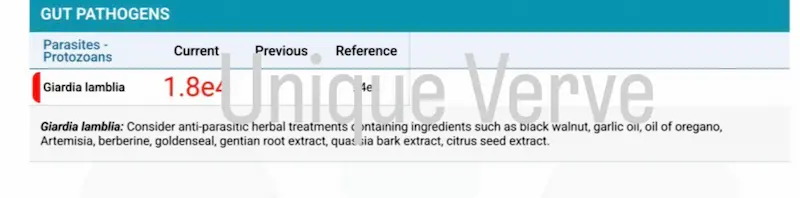
The comprehensive testing we ran revealed one of the most complex upstream pictures I have encountered. Her CBC with differential showed clinically elevated eosinophils — a white blood cell pattern indicative of parasitic infection. Her Gut Zoomer confirmed high levels of parasites alongside significant dysbiosis, providing the mechanism for her severely impaired DAO production and the chronic gut inflammation driving her daily diarrhea and stomach pain.
Her Wheat Zoomer revealed severe leaky gut alongside high levels of anti-LPS antibodies — confirming that bacterial fragments were actively entering her circulation and triggering systemic immune activation. The LPS translocation was crossing her blood-brain barrier and driving neuroinflammation — which explained the severity and character of her mood symptoms, irritability, brain fog, and emotional reactivity in a way that no psychiatric assessment had been able to account for.
Her Total Tox Burden panel revealed extreme toxic burden across all three categories simultaneously — mycotoxins, environmental chemicals, and heavy metals. This toxic overload was maintaining her immune system in a state of chronic hypervigilance, amplifying her histamine bucket continuously regardless of what she ate or avoided.
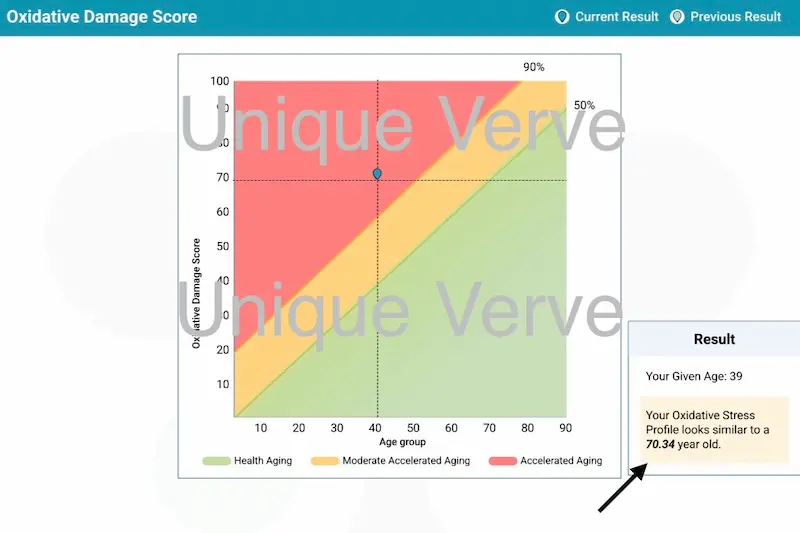
The most striking finding was her Vibrant Wellness Oxidative Stress Profile — a panel that assesses your DNA’s capacity to biotransform harmful substances and the genetic variants affecting your most powerful intracellular antioxidant systems. Her results showed blockages and genetic SNPs at every step of the detoxification process, involving the most critical intracellular antioxidants — glutathione and superoxide dismutase. Her biological age as assessed by this panel was 70.34 years against her actual age of 39. Every genetic detoxification pathway was compromised, meaning her body’s demands for nutrients to support detoxification and histamine degradation were extraordinarily high — while her daily diarrhea was simultaneously depleting the very nutrients those pathways required to function.
She later reported that she had experienced parasites in childhood as well — suggesting a lifelong history of gut immune compromise that had never been fully addressed, and that had created the conditions for the compounding toxic, hormonal, and histamine picture that was now producing her full symptom spectrum at 38.
Her protocol addressed every upstream driver systematically — parasitic and gut infection clearance, gut lining restoration, toxin biotransformation/detoxification support, targeted nutrient repletion for her specific genetic detoxification vulnerabilities, hormonal rebalancing and thyroid optimization. The diarrhea resolved. The stomach pain cleared. Her mood stabilized. The brain fog lifted. The irritability and emotional reactivity that had been present her entire adult life reduced to a level she had never experienced before. Her PMS symptoms gone.
Most recently, she reported something that crystallized the whole picture: before we began working together, she used to get sick frequently — repeated infections that she had normalized as just part of her life. She no longer gets sick. Her immune system, no longer consumed by the parasitic burden, the toxic overload, and the histamine hypervigilance that had kept it in a state of chronic activation, now has the resources and the regulatory capacity to perform its primary protective function.
This case illustrates what is achievable when the full upstream picture is investigated and addressed — not just the symptoms that have been labeled, but the interconnected drivers that conventional medicine’s organ-by-organ approach was structurally unable to connect.
The Low-Histamine Diet: A Supportive Tool, Not a Solution
A low-histamine diet — reducing high-histamine foods including aged cheeses, fermented foods, alcohol, processed meats, vinegar, and certain vegetables and fruits — can provide meaningful symptomatic relief by reducing the dietary contribution to the histamine bucket while upstream work is underway. For some patients, temporary dietary modification reduces the symptom burden enough to allow the functional medicine protocol to make progress without the constant immune activation of a bucket that is chronically overflowing.
However, a low-histamine diet addresses only one input into the histamine bucket and does nothing to address the impaired degradation capacity that is allowing the bucket to overflow in the first place. A patient with dysbiosis, parasitic infection, extreme toxic burden, genetic detoxification vulnerabilities, and estrogen dominance will not resolve her histamine intolerance through dietary management — because the primary drivers of her histamine overload are internal, systemic, and largely independent of food intake. Restricting diet indefinitely while leaving these upstream drivers unaddressed produces partial and temporary relief while the underlying picture continues to progress.
This is the most important caveat about the low-histamine diet: it is a supportive tool for symptom management during the period when upstream drivers are being identified and addressed. It is not a treatment for histamine intolerance. And for many patients, the dietary restrictions required to manage symptoms through food alone are so extensive that they produce nutritional insufficiencies that worsen the very DAO cofactor depletion contributing to the problem.
Testing: Building the Histamine Intolerance Picture Without a Direct DAO Measurement
Building the clinical picture of signs and symptoms of histamine intolerance without a direct DAO measurement requires targeted testing of the upstream drivers producing the histamine excess.
Because DAO enzyme activity is not captured in standard blood panels and histamine levels fluctuate too rapidly to be reliably measured in a single draw, the functional medicine approach to histamine intolerance builds the picture indirectly through targeted testing of the upstream drivers. Every workup is individualized based on health history and symptom presentation. The panels most consistently relevant include:
CBC with differential — eosinophil levels provide a direct indicator of parasitic or allergic immune activation that is contributing to histamine overload. This is one of the most accessible and most informative initial markers in a histamine intolerance workup.
Gut Zoomer — comprehensive stool test and microbiome assessment identifying dysbiosis, pathogen burden including parasites, candida overgrowth and SIBO. The gut picture almost always contains the primary mechanism of DAO impairment.
Wheat Zoomer — anti-LPS antibodies confirming gut bacterial translocation into circulation and the degree of intestinal permeability driving systemic immune activation.
Total Tox Burden — heavy metals, mycotoxins, and environmental chemicals. Given the central role of toxic overload in priming immune hypervigilance and impairing detoxification pathways, this panel is essential when toxic exposure is part of the clinical picture.
Micronutrient Panel with SNPs — cellular levels of B6, vitamin C, copper, and other DAO cofactors alongside the genetic variants affecting how nutrients are absorbed, utilized, and how detoxification pathways function. The Oxidative Stress Profile assesses genetic detoxification capacity specifically.
Hormone Zoomer — 24-hour urinary estrogen metabolites and clearance pathways, progesterone, and cortisol. The hormonal picture determines how much estrogen-driven mast cell stimulation is contributing to histamine production.
Full thyroid panel — TSH, free T3, free T4, reverse T3, and both antibodies. The thyroid-TBG-histamine connection makes thyroid assessment non-negotiable in any comprehensive histamine intolerance workup.
Do Not Ignore Your Symptoms — They Will Not Improve on Their Own
Aging accelerates aging. Every year that the upstream drivers of histamine intolerance remain unaddressed, the picture becomes more entrenched, more complex, and harder to reverse. The window for intervention is now — not after perimenopause makes every driver harder to manage simultaneously.
Before addressing what to do, it is worth establishing something that gets lost in the conventional histamine conversation: histamine is not the enemy. It is an essential biological mediator required for a remarkably broad spectrum of functions — stomach acid production, blood pressure regulation, blood-brain barrier protection, muscle function, systemic response to exercise, immune activation, inflammation and phagocytosis, chemosensory behavior, and glucose uptake. The goal is never to suppress histamine. The goal is to restore the body’s capacity to produce and degrade it in appropriate balance — so that it continues performing its essential biological functions without accumulating to the level that produces the symptom picture described throughout this post.
Antihistamines suppress the downstream signal without addressing the upstream imbalance — and their long-term consequences go further than most patients are told. Ongoing antihistamine use progressively worsens allergic reactivity by upregulating histamine receptor sensitivity in response to chronic receptor blockade. Long-term use has been associated with increased risk of dementia and glioma.
Antihistamines also deplete essential fatty acids — the very nutrients required for healthy cell membrane function in every cell and organ in the body, including the skin, where they maintain the acid mantle and barrier integrity. Essential fatty acid depletion is itself associated with the inflammatory skin conditions — rosacea, eczema, acne, psoriasis, dermatitis — that histamine overload was already driving. The result is a vicious cycle: antihistamines suppress histamine symptoms while depleting the very nutrients needed to maintain the skin barrier and membrane integrity that histamine overload was compromising in the first place — and the skin condition the antihistamine was never treating continues to worsen.
Any drug that chronically blocks a receptor for an innate biological substance deprives the body of its beneficial actions simultaneously — which is why antihistamine dependency is not a management strategy, it is a compounding problem.
This is where functional medicine offers something fundamentally different: not a strategy to manage one symptom in isolation, but a single strategic treatment plan designed to bring your entire biochemistry back into homeostasis — addressing your allergies, gut issues, skin conditions, heart palpitations, and mood imbalances simultaneously, because they were never separate problems to begin with. Your symptoms deserve investigation, not suppression.
I want to say this directly to every woman who has been dismissed, told her results are normal, or given a partial diagnosis that explains only one aspect of her symptom picture: your symptoms are real, they are connected, and they are telling you something important about what is happening upstream in your body. Do not normalize them. Do not wait for them to become severe enough to be taken seriously by conventional medicine. And do not manage them indefinitely with antihistamines, antidepressants, or elimination diets that address the downstream expression while the upstream cause continues to progress.
The signs and symptoms of histamine intolerance do not resolve on their own — they accumulate, compound, and become progressively more entrenched with each year the upstream drivers remain unaddressed.
Entering perimenopause with unaddressed histamine intolerance and its upstream drivers amplifies every aspect of the picture. Perimenopause suppresses innate immune function and predisposes women to recurrent infections — UTIs, respiratory illness, and viral susceptibility that reflect the immune resource depletion that chronic histamine activation has been producing for years. The insulin resistance of perimenopause worsens blood sugar dysregulation that feeds gut pathogens and impairs DAO production. Declining thyroid function amplifies the toxic burden cycle. And the hormonal shift that removes progesterone’s mast cell-stabilizing effect removes the last biological brake on the histamine picture that was keeping symptoms manageable.
The toxic overload component carries an additional consequence that is rarely discussed: chronic toxic burden contributes to earlier onset of perimenopause and menopause by disrupting hormonal signaling and accelerating ovarian aging. A woman who enters perimenopause with significant toxic burden may do so years earlier than her biology would otherwise dictate — and with an immune system, a gut, and a detoxification capacity that are already significantly depleted.
Functional medicine is a complementary approach to conventional medicine — not a replacement for it. The diagnostic tools, specialist care, and acute management that conventional medicine provides are valuable and sometimes essential. What functional medicine adds is the upstream investigation that conventional medicine’s organ-by-organ structure is not designed to perform: identifying the interconnected drivers that produce the symptom pattern, addressing them in the right sequence, and restoring the body’s own regulatory capacity so that the symptoms resolve rather than being managed indefinitely.
The patient case I shared today is a real example of what that investigation reveals and what it makes possible. A woman who had lived with daily diarrhea, mood dysregulation, and frequent illness since childhood — whose biological age at 38 was assessed at over 70 — who now no longer gets sick, whose gut is calm, whose mood is stable, and whose body is rebuilding from a depleted baseline toward the vitality her actual age should represent.
Your symptom picture is not random. It is not anxiety. It is not aging. It is a signal. And it deserves a clinical framework that is actually designed to listen to it.
P.S. If finances have been the only thing standing between you and starting your functional medicine journey — flexible payment options are available through Cherry. No interest, no impact on your credit score, quick approval, and affordable monthly payments — available for functional medicine programs, lab testing, supplements, and Environ skincare. Apply in minutest here.
Frequently Asked Questions
Q1: How do I know if I have histamine intolerance?
Histamine intolerance does not have a single identifiable symptom — it produces a broad, multi-system picture that spans skin, gut, cardiovascular, neurological, mood, hormonal, and respiratory systems simultaneously. The most clinically significant pattern is symptoms across multiple organ systems that have not responded to conventional treatment for each individual system, alongside a history of reactions that feel inconsistent and unpredictable. Common presentations include urticaria, flushing, rosacea, dermatitis or eczema alongside gut symptoms like bloating, diarrhea, or nausea, alongside mood symptoms like anxiety, irritability, or brain fog, alongside cardiovascular symptoms like palpitations or elevated heart rate. If your symptom picture spans multiple systems and your conventional testing has returned normal, histamine intolerance is worth investigating through a functional medicine lens.
Q2: Why can’t my doctor find what’s wrong?
Because histamine intolerance has no official disease label in conventional medicine — and without a label, there is no billing code, no standard diagnostic protocol, and no specialist whose remit it falls within. Conventional medicine’s organ-by-organ specialty structure routes each symptom to a different department: dermatology for the skin, gastroenterology for the gut, cardiology for the palpitations, psychiatry for the mood symptoms. Nobody in any of those appointments is positioned to connect them as expressions of a single systemic pattern. Additionally, DAO enzyme activity — the primary degradation pathway for histamine — is not measured in standard blood panels, and histamine levels fluctuate too rapidly to be reliably captured in a single draw. Functional medicine looks at the symptom pattern, the upstream drivers, and the interconnectedness of systems rather than requiring a disease label to validate an investigation.
Q3: Why do I feel worse after eating?
Post-meal worsening of symptoms is one of the most consistent presentations of histamine intolerance. High-histamine foods — aged cheeses, fermented foods, alcohol, processed meats, vinegar, and certain fruits and vegetables — add directly to the histamine bucket. But even foods that are not particularly high in histamine can trigger symptoms in patients with significantly impaired DAO enzyme function, because the gut’s capacity to degrade dietary histamine before it reaches circulation is so compromised that normal histamine loads produce an overflow response. Post-meal symptoms that worsen in the evening — when histamine from the day’s food intake has accumulated alongside the histamine produced by gut bacteria and mast cell activation throughout the day — are particularly characteristic of a chronically full histamine bucket.
Q4: Is my rash or skin reaction from histamine intolerance?
Possibly — and if you also have gut symptoms, mood symptoms, or cardiovascular symptoms alongside your skin reactions, the probability increases significantly. Histamine activates mast cells densely distributed throughout the skin, producing urticaria, pruritus, flushing, redness, and inflammatory skin conditions including rosacea, eczema, and acne. Skin reactions that appear unpredictably, worsen cyclically with the menstrual cycle, respond partially to antihistamines, or occur alongside digestive or mood symptoms strongly suggest a histamine-driven picture rather than a purely topical skin condition. The gut-skin connection in histamine-driven skin conditions is explored in depth in our rosacea cluster — the same upstream picture driving urticaria and rosacea is almost always present together in clinical practice.
Q5: Can stress make histamine intolerance symptoms worse?
Yes — significantly, and through a direct biochemical mechanism. Stress depletes vitamin B6 and vitamin C — the primary cofactors required for DAO enzyme activity. When these nutrients are depleted through chronic stress, the gut’s histamine degradation capacity is reduced regardless of gut lining integrity or dysbiosis status. Cortisol elevation from chronic stress also increases thyroid hormone binding globulin (TBG), reducing free thyroid hormone availability and impairing the gut motility, DAO production, and detoxification capacity that thyroid hormone supports. The result is that a high-stress period directly increases the histamine bucket fill rate while simultaneously reducing the drainage rate — producing symptom flares that appear to have no dietary or environmental trigger because the trigger is internal and metabolic.
Q6: Is my bloating related to histamine intolerance?
Bloating is one of the most consistent gut symptoms of histamine intolerance — produced through histamine’s direct effects on gut motility, gastric acid secretion, and gut smooth muscle tone. Histamine H2 receptor activation in the stomach increases gastric acid secretion, which can produce the reflux, burping, and digestive discomfort that accompanies histamine-driven bloating. When gut dysbiosis is the primary upstream driver — through histamine-producing bacteria, SIBO, or parasitic infection impairing DAO production — the bloating is produced by both the dysbiosis itself and the histamine excess it creates simultaneously. Bloating that worsens in the second half of the menstrual cycle, in high-stress periods, or in response to a broad range of foods rather than specific identifiable triggers is particularly suggestive of a histamine-driven picture.
Q7: Is my insomnia related to histamine?
Yes — and the mechanism is direct. Histamine is a wakefulness-promoting neurotransmitter in the brain — histaminergic neurons in the hypothalamus promote arousal and wakefulness through H1 receptor activation. In histamine intolerance, elevated systemic histamine crosses the blood-brain barrier and activates these wakefulness pathways at times when they should be quiescent — producing the difficulty falling asleep, middle-of-the-night waking, and non-restorative sleep that are among the most consistent neurological signs and symptoms of histamine intolerance. The insomnia of histamine excess is characteristically worse on high-histamine eating days, in the luteal phase of the menstrual cycle when estrogen-driven mast cell activation is highest, and during periods of high stress when B6 depletion reduces histamine degradation capacity.
Q8: Why am I suddenly sensitive to everything?
Global reactivity — becoming sensitive to an expanding range of foods, products, environments, and stressors that were previously tolerated — is one of the most diagnostically significant patterns in histamine intolerance. It reflects a histamine bucket that is chronically full, leaving the immune system in a state of permanent hypervigilance where the threshold for mast cell activation is extremely low. When the bucket is chronically full, even small additional inputs — a food that was previously tolerated, a fragrance, a temperature change — produce overflow reactions because the system is already at capacity. Progressive sensitivity expansion over time almost always indicates that the upstream drivers filling the bucket are increasing in burden rather than being addressed — which is why the trajectory of histamine intolerance without upstream intervention is consistently one of progressive worsening.
Q9: Is histamine intolerance permanent or reversible?
Histamine intolerance is not a permanent condition — it is a state of histamine excess relative to degradation capacity that can be meaningfully improved and in many cases resolved when the upstream drivers are comprehensively identified and addressed. DAO enzyme production can be restored as gut lining integrity improves. Nutrient cofactors for DAO activity can be repleted. Toxic burden can be reduced. Hormonal balance can be restored. Thyroid function can be optimized. The extent and pace of improvement depends on the complexity and duration of the upstream picture, the presence of genetic detoxification vulnerabilities, and how consistently the protocol is maintained. The most important determinant of outcome is how early the upstream investigation begins — which is why not ignoring symptoms and not waiting for the picture to worsen is the single most important clinical recommendation I can make.
Q10: Why does mold make me feel sick with histamine symptoms?
Mycotoxins from mold exposure are one of the most potent upstream triggers of histamine hyperreactivity. Mycotoxins prime the immune system for chronic hypervigilance by maintaining a state of low-grade immune activation that keeps mast cells primed for degranulation — meaning that even ordinary histamine inputs produce outsized reactions. Mycotoxin exposure also impairs the liver’s CYP450 biotransformation pathways that are needed to clear both the toxins and histamine metabolites — creating the vicious cycle of toxin accumulation, impaired clearance, increasing immune hypervigilance, and worsening histamine reactivity. The Total Tox Burden panel identifies mycotoxin burden specifically and is one of the most clinically important tests in a histamine intolerance workup when mold exposure is part of the history.
Written by Natalie Maibenko – a Certified Functional Medicine Practitioner and Master Esthetician with 22+ years of experience and founder of Unique Verve

As a Certified Functional Medicine Practitioner my Expertise Encompasses:
- Immune System: frequent illness, UTIs, yeast infections
- Allergies, Asthma
- Skin Problems: acne, cystic acne, rosacea, eczema, dermatitis, ichthyosis, psoriasis, vitiligo, melasma
- Inflammation: arthritis, rhinitis, joint & muscle pain, migraines, headaches
- Sleep Disturbunces, Insomnia
- Gut Problems: IBS/IBD, bloating, acid reflux, gas, constipation, diarrhea, parasites, fungal/yeast overgrowths
- Hormonal Imbalances: PCOS, PMS symptoms, weight problems/inability to lose weight, thyroid problems
- Hair Loss, Alopecia
- Mood Imbalances: anxiety, depression, irritability
- Metabolic Dysfunction, Insulin Resistance, Type 2 Diabetes
- Optimizing Wellness for Successful Pregnancy
- Autoimmune Conditions: Hashimoto’s thyroiditis, grave’s disease, reumatoid arthritis (RA), lupus, etc
- Bone Health: osteopenia/ osteoporosis
- Effective Anti-Aging Strategies without Injectables with the inside-out & outside-in approach
- Detoxification of Heavy Metals, Mycotoxins, Environmental Toxins
- Reversing Breast Implant Illness
- Preparation for the Explant Surgery and Optimization of Wellness & Vitality Post-Explant
With love and gratitude,
Natalie Maibenko
Functional Medicine & Skincare Expert – Helping You Take Control of Your Health and Achieve Lasting Skin Results Nationwide — Virtual Practice