Introduction
Rosacea and autoimmune diseases share more than a clinical profile of persistent inflammation and female predominance. Research increasingly confirms that the two are connected through shared genetic risk loci, overlapping upstream immune drivers, and a documented statistical association that no rosacea patient should be unaware of — not because the connection is alarming, but because understanding it changes what upstream investigation is most important and why the window for intervention matters.
The most important clinical reframe is this: rosacea and autoimmune diseases are not separate conditions that happen to sometimes co-occur. They reflect different expressions of the same underlying immune dysregulation terrain, activated by the same upstream drivers — subclinical thyroid dysfunction, gut dysbiosis, toxic burden, hormonal imbalance, and viral triggers — in people who carry a shared genetic susceptibility for inflammatory and autoimmune conditions. What differentiates the rosacea patient from the celiac or rheumatoid arthritis patient is not the upstream environment. It is which genetic susceptibility that environment has activated so far.
This post covers what the research actually shows about rosacea and autoimmune diseases, why the female predominance of both is not coincidental, what the epigenetic triggers are that tip the immune system from rosacea-level dysregulation toward true autoimmune tissue targeting, and why the window for rosacea root-cause upstream investigation matters more than any label that might eventually apply.
Rosacea and Autoimmune Diseases: What the Research Actually Shows
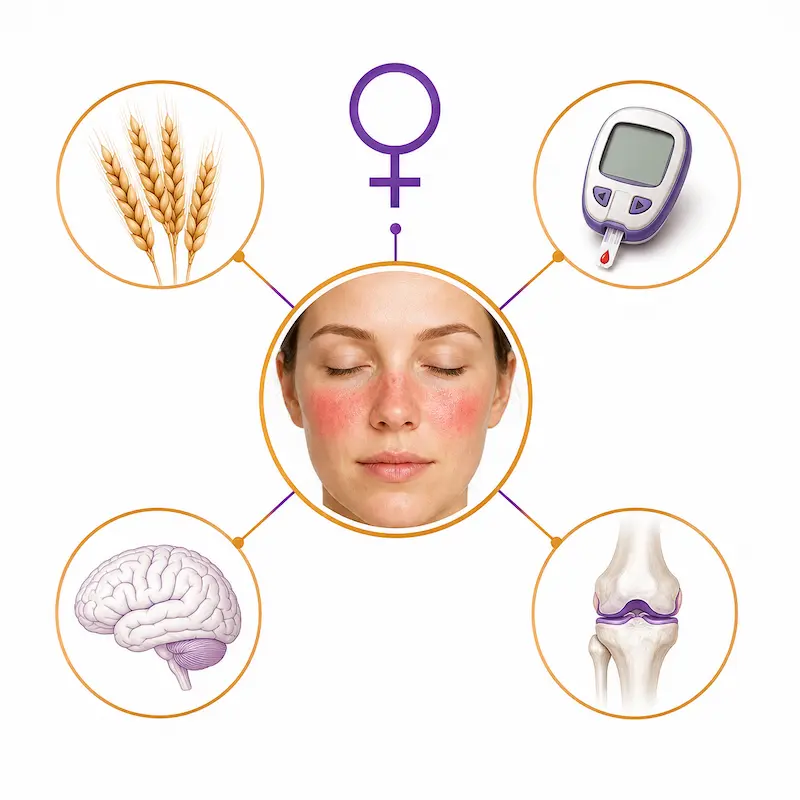
A large population-based case-control study published in the Journal of the American Academy of Dermatology examined the association between rosacea and four specific autoimmune conditions in 6,759 rosacea patients matched against 33,795 controls. The findings were striking and specific: rosacea was significantly associated with type 1 diabetes mellitus, celiac disease, multiple sclerosis, and rheumatoid arthritis — and this association was statistically significant specifically in women, while in men only the association with rheumatoid arthritis reached significance.
The research also confirmed that rosacea shares genetic risk loci with these autoimmune conditions — specific regions of the genome associated with susceptibility to T1DM, celiac disease, multiple sclerosis, and rheumatoid arthritis are also found in rosacea susceptibility profiles. This genetic overlap does not mean autoimmune progression is inevitable. It means the same genetic terrain that allowed rosacea to develop carries the raw material for these conditions to emerge if the internal environment activates them.
A separate body of research documents the thyroid autoimmunity connection specifically. Rosacea patients show significantly elevated thyroid autoantibodies, increased rates of hypothyroidism peaking in the 40-49 age range, and structural thyroid changes including larger nodules and more heterogeneous thyroid tissue compared to non-rosacea controls. Research following over 15,000 Hashimoto’s thyroiditis patients found they carried a significantly increased risk of developing subsequent systemic lupus erythematosus — creating a documented progression pathway from rosacea-adjacent immune dysregulation through thyroid autoimmunity toward lupus risk.
Standard blood tests used in conventional medicine are not designed to detect this picture. A TSH within the conventional normal range does not rule out occult Hashimoto’s thyroiditis — up to 30% of patients with TSH above 3.0 mU/L have autoimmune thyroid disease that TSH-only testing never captures. Rosacea and its autoimmune associations live in the gap between what standard testing measures and what functional medicine investigates.
Why Women Are Disproportionately Affected
The female predominance of both rosacea and autoimmune diseases reflects a convergence of biological mechanisms that functional medicine is positioned to investigate and address. A cross-sectional study of 3,397 elderly individuals confirmed significant sexual dimorphism in thyroid health — women had 2.3 times the risk of positive thyroid antibodies and 1.79 times the risk of thyroid dysfunction compared to men, with this disparity consistent across all iodine nutrition levels. This is a fundamental difference in immune regulation between male and female physiology.
Estrogen directly stimulates mast cells and drives histamine production. Progesterone stabilizes mast cells and provides immune regulatory counterbalance. As progesterone begins its perimenopausal decline — which can start as early as the mid-30s — the relative estrogen dominance that results simultaneously amplifies the mast cell activation driving rosacea, reduces the immune regulatory capacity preventing autoimmune progression, and increases susceptibility to the viral and metabolic triggers most consistently associated with autoimmune expression.
The perimenopause years are therefore not just a period of hormonal transition. They are the period of maximum autoimmune vulnerability for the woman who has been carrying unaddressed rosacea upstream drivers for years — which is why the statistical peak for hypothyroidism in rosacea patients falls precisely in the 40-49 age range, and why so many women experience their rosacea worsening most significantly at exactly this stage of life.
Genetics Load the Gun. Epigenetic Triggers Pull It.
The shared genetic risk loci between rosacea and autoimmune conditions create susceptibility — but susceptibility is not destiny. Functional medicine understands genetic predisposition as raw material that requires an environmental trigger to express. The same internal environment that allowed rosacea to develop may, if the right combination of triggers converges, activate the genetic predisposition for celiac, T1DM, MS, or RA in a person who had the potential for those conditions all along.
The most consistently significant epigenetic tipping point in clinical practice is subclinical hypothyroidism — thyroid function suboptimal by functional medicine standards but within the conventional normal range. When subclinical hypothyroidism coincides with any combination of the following triggers, the internal environment can cross the threshold from immune-mediated rosacea into true autoimmune progression:
Viral Reactivation
Because rosacea involves significant immune dysregulation, patients with chronic rosacea are operating with depleted immune regulatory capacity, making them more susceptible to viral triggers. In clinical practice, consistent co-occurrence is seen with Epstein-Barr Virus reactivation, herpes simplex reactivation, and COVID-19 infection. COVID-19 specifically triggers aggressive IL-17 pro-inflammatory cytokine elevation — a pathway directly implicated in rosacea pathogenesis — and downregulates ACE2 receptors, amplifying the inflammatory cascade driving both rosacea flares and systemic immune dysregulation. A cross-sectional study of 104 rosacea patients found that 28.8% experienced rosacea exacerbation after COVID-19 infection and 15.4% after vaccination, with metabolic comorbidities significantly increasing the risk.
Toxic Overload
Heavy metal burden, mycotoxin exposure, and environmental chemical accumulation prime the immune system for chronic hypervigilance while impairing the detoxification and nutrient absorption capacity needed for immune regulatory function. Mercury specifically has been documented in case studies to produce autoimmune presentations indistinguishable from lupus and rheumatoid arthritis, and is directly linked to thyroid autoimmunity that increases subsequent lupus risk. When toxic burden is accumulating while subclinical hypothyroidism impairs the detoxification capacity needed to clear it, the self-reinforcing cycle creates conditions for autoimmune genetic expression.
Gut Dysbiosis
The gut is where approximately 70% of immune regulation occurs. Gut dysbiosis, leaky gut, H. Pylori infection, and parasitic burden each impair the Treg regulatory capacity that prevents autoimmune tissue targeting, while simultaneously producing the molecular mimicry risk and chronic LPS-driven immune activation that can tip the immune system toward autoimmune progression. In the rosacea patient with unresolved gut dysbiosis, the gut is not only producing histamine and impairing DAO — it is actively eroding the immune regulatory infrastructure that separates immune-mediated rosacea from true autoimmune disease.
The Pattern I Consistently See
Across patients presenting with rosacea alongside symptoms suggesting early autoimmune progression — joint pain, significant fatigue, thyroid antibody elevation, gut dysfunction, recurrent illness, and mood dysregulation — the functional medicine investigation reveals a consistent upstream picture. Subclinical thyroid dysfunction present in virtually every case, frequently with elevated anti-TPO or anti-thyroglobulin antibodies that TSH-only testing never captures. Significant gut dysbiosis — often including H. Pylori, parasitic infection, or SIBO — impairing the gut-immune regulatory capacity that prevents autoimmune progression. Total Tox Burden findings showing heavy metal, mycotoxin, and environmental chemical burden maintaining the immune system in a state of chronic hypervigilance. Nutrient insufficiencies — particularly vitamin A, D3, zinc, and omega-3 fatty acids — depleting the Treg cofactors needed for immune self-tolerance.
None of these findings are rare. All of them are measurable. And all of them are addressable through targeted intervention — which is the clinical point that the rosacea and autoimmune diseases question most needs to land on. Yes, the research confirms the association and the progression risk. But the progression is not inevitable. It reflects an upstream environment that can be investigated, addressed, and in many cases significantly improved before the genetic susceptibility for these conditions is fully expressed.
The Urgency of Investigation
Rosacea and autoimmune diseases share an upstream origin. The label — rosacea, celiac, Hashimoto’s, rheumatoid arthritis — tells you where the immune system’s current target is. The upstream investigation tells you why. And addressing the why is what makes it possible for the where to change.
Once autoimmune progression begins, it tends to cascade. Patients with one autoimmune condition carry significantly elevated risk of developing secondary and tertiary autoimmune conditions — because the upstream environment that produced the first has not been addressed and the immune regulatory capacity that might have contained it is already depleted. Hashimoto’s thyroiditis specifically carries downstream consequence for every cell in the body, since thyroid hormone is responsible for cellular respiration — the metabolic foundation of every physiological function.
Entering perimenopause with unaddressed rosacea upstream drivers accelerates every aspect of this picture simultaneously. The hormonal shift removes the mast cell-stabilizing effect of progesterone. Insulin sensitivity worsens. Immune competence declines. Detoxification slows. And the toxic burden that has been accumulating may be accelerating perimenopause onset itself — an additional downstream consequence of the same upstream environment that has been driving the rosacea.
Functional medicine does not treat the label. It treats the person — the symptoms that are present, the history of what has happened over a lifetime, the precipitating factors and contributors that created the tipping point, and the upstream drivers that are sustaining the dysregulation. The label tells you where. The upstream investigation tells you why. And the functional medicine program addresses the why — which is the only intervention that actually changes the trajectory.
→ Book your Initial Functional Medicine Health and Skin Assessment
P.S. If finances have been the only thing standing between you and starting your functional medicine journey — flexible payment options are available through Cherry. No interest, no impact on your credit score, quick approval, and affordable monthly payments. Apply in minutes on our website.
Frequently Asked Questions
Q1: What autoimmune disease is associated with rosacea?
Research has identified four specific autoimmune conditions that are statistically associated with rosacea: type 1 diabetes mellitus, celiac disease, multiple sclerosis, and rheumatoid arthritis. These associations were found to be significant specifically in women in a large population-based case-control study. Rosacea also shares genetic risk loci with all four conditions, suggesting a common upstream immune susceptibility terrain. Beyond these four, rosacea is associated with elevated thyroid autoantibodies and increased rates of Hashimoto’s thyroiditis — which itself carries increased risk for subsequent lupus development. The common thread across all of these associations is not the conditions themselves but the shared upstream environment of immune dysregulation, gut dysfunction, toxic burden, and hormonal imbalance that allows both rosacea and autoimmune conditions to develop in susceptible individuals.
Q2: Can blood tests detect rosacea autoimmune disease connection?
Standard blood tests are not designed to detect the rosacea-autoimmune connection — which is why so many rosacea patients are told their results are normal while their symptoms continue to progress. TSH-only thyroid testing misses occult Hashimoto’s thyroiditis in up to 30% of patients with TSH above 3.0 mU/L. Standard metabolic panels miss early insulin resistance when fasting insulin is not run alongside glucose and HbA1C. No standard panel tests for gut microbiome status, intestinal permeability, parasitic burden, heavy metal accumulation, or mycotoxin exposure — the findings most consistently relevant to rosacea’s autoimmune association. The functional medicine workup that reveals this picture includes full thyroid panel with both anti-TPO and anti-thyroglobulin antibodies simultaneously, Gut Zoomer, Total Tox Burden, Micronutrient Panel with SNPs, and Hormone Zoomer. Each of these panels investigates the upstream environment that standard testing does not reach.
Q3: Does having rosacea increase my risk of developing autoimmune diseases?
Research confirms that rosacea is statistically associated with increased risk of type 1 diabetes, celiac disease, multiple sclerosis, and rheumatoid arthritis — particularly in women. This does not mean autoimmune progression is inevitable. The association reflects shared genetic susceptibility and a common upstream immune dysregulation environment. Whether that susceptibility is expressed as additional autoimmune conditions depends significantly on the internal environment — the state of thyroid function, gut integrity, toxic burden, nutrient sufficiency, and hormonal balance. Addressing these upstream factors through functional medicine investigation is the most proactive intervention available for a rosacea patient who wants to reduce her autoimmune progression risk rather than wait for a diagnosis to confirm it.
Q4: Why do I have both rosacea and an autoimmune condition like Hashimoto’s or RA?
Because both conditions reflect the same upstream immune dysregulation environment expressing through different genetic pathways simultaneously. The gut dysfunction, toxic burden, hormonal imbalance, nutrient insufficiency, and subclinical thyroid dysfunction that created the conditions for rosacea to develop are the same factors that activated the genetic susceptibility for Hashimoto’s, rheumatoid arthritis, or any other autoimmune condition co-occurring alongside it. They are not separate problems that happen to coexist — they are parallel expressions of the same upstream picture. The functional medicine approach therefore investigates and addresses the shared root cause environment rather than treating each condition in isolation, which is why functional medicine interventions tend to produce improvements across multiple conditions simultaneously rather than managing each one independently.
Q5: Can rosacea cause other health problems beyond the skin?
Yes — and the research supports this at multiple levels. Rosacea is associated with elevated rates of cardiovascular disease markers, gut dysfunction including altered microbiome composition and increased intestinal permeability, neurological symptoms including anxiety and depression driven by the same neuroinflammatory pathways involved in rosacea, and the autoimmune conditions discussed throughout this post. The systemic picture of rosacea reflects the reality that what appears on the skin is the visible expression of immune dysregulation that is simultaneously affecting the gut, the thyroid, the cardiovascular system, and the nervous system. This systemic picture is explored in greater depth in our dedicated post on how rosacea affects more than the skin.
Q6: Will my rosacea get progressively worse if I don’t address the root cause?
In clinical experience, yes — consistently. The upstream drivers of rosacea — gut dysbiosis, subclinical thyroid dysfunction, toxic burden, nutrient depletion, and hormonal imbalance — do not resolve on their own and tend to become more entrenched over time as each driver compounds the others. The gut damage that impairs nutrient absorption worsens the nutrient insufficiency that impairs gut repair. The thyroid insufficiency that slows detoxification worsens the toxic burden that impairs thyroid function. Without upstream investigation and targeted intervention, the internal environment driving rosacea continues to develop — and the threshold for immune reactivity lowers progressively, making the condition harder to address and the risk of autoimmune progression higher with each year that passes.
Written by Natalie Maibenko – a Certified Functional Medicine Practitioner and Master Esthetician with 22+ years of experience and founder of Unique Verve

As a Certified Functional Medicine Practitioner my Expertise Encompasses:
- Immune System: frequent illness, UTIs, yeast infections
- Allergies, Asthma
- Skin Problems: acne, cystic acne, rosacea, eczema, dermatitis, ichthyosis, psoriasis, vitiligo, melasma
- Inflammation: arthritis, rhinitis, joint & muscle pain, migraines, headaches
- Sleep Disturbunces, Insomnia
- Gut Problems: IBS/IBD, bloating, acid reflux, gas, constipation, diarrhea, parasites, fungal/yeast overgrowths
- Hormonal Imbalances: PCOS, PMS symptoms, weight problems/inability to lose weight, thyroid problems
- Hair Loss, Alopecia
- Mood Imbalances: anxiety, depression, irritability
- Metabolic Dysfunction, Insulin Resistance, Type 2 Diabetes
- Optimizing Wellness for Successful Pregnancy
- Autoimmune Conditions: Hashimoto’s thyroiditis, grave’s disease, reumatoid arthritis (RA), lupus, etc
- Bone Health: osteopenia/ osteoporosis
- Effective Anti-Aging Strategies without Injectables with the inside-out & outside-in approach
- Detoxification of Heavy Metals, Mycotoxins, Environmental Toxins
- Reversing Breast Implant Illness
- Preparation for the Explant Surgery and Optimization of Wellness & Vitality Post-Explant
With love and gratitude,
Natalie Maibenko
Functional Medicine & Skincare Expert – Helping You Take Control of Your Health and Achieve Lasting Skin Results Nationwide — Virtual Practice