Introduction
Why is my rosacea getting worse — despite doing everything your dermatologist suggested? Despite the antibiotics, the azelaic acid, the trigger avoidance, and the reassurance that your blood tests are normal? This is one of the most common and most frustrating clinical presentations I encounter: a patient whose rosacea is demonstrably progressing, whose conventional workup has returned consistently normal, and who has been given no explanation for why the condition keeps worsening despite compliant treatment.
The answer — almost universally — is that the tests being run are not designed to find what is driving rosacea. Not because the tests are wrong, but because the question being asked by conventional medicine is the wrong question. “Is there diagnosable pathology?” is a different question from “what is creating the internal environment in which rosacea develops, progresses, and resists treatment?” Standard blood panels answer the first question. Functional medicine investigates the second.
This post explains why “normal” on a standard panel is not the same as “optimal” or “nothing is wrong,” what the functional medicine rosacea root cause investigation actually measures that standard testing misses entirely, what specific factors cause rosacea to suddenly worsen after a period of relative stability, and why the longer the upstream picture goes uninvestigated the more entrenched and harder to reverse rosacea becomes.
Why Is My Rosacea Getting Worse When My Tests Are Normal? What “Normal” Actually Means
The reference ranges that define “normal” on a standard blood panel are built from population statistics — specifically, the results of approximately 95% of the people who were tested when the ranges were established. Normal means average. And in the United States, average does not mean healthy.
Research published in Metabolic Syndrome and Related Disorders found that only 6.8% to 12.2% of American adults have optimal metabolic health — even among normal weight individuals. This means that nearly 93% of US adults have some level of metabolic dysfunction. When the reference range for “normal” blood glucose, insulin, or inflammatory markers is built from a population in which 93% are metabolically compromised, a result that falls within that range is not evidence of optimal health. It is evidence of being average in a population that is largely unwell.
Functional medicine reference ranges are different. They are built around optimal function — the values associated with the lowest disease risk and the highest physiological resilience — rather than around population averages. This distinction is not semantic. For a rosacea patient whose conventional panel consistently returns normal, it is the difference between “there is nothing to investigate” and “there is a specific picture of suboptimal function that is creating the internal environment driving your skin inflammation.”
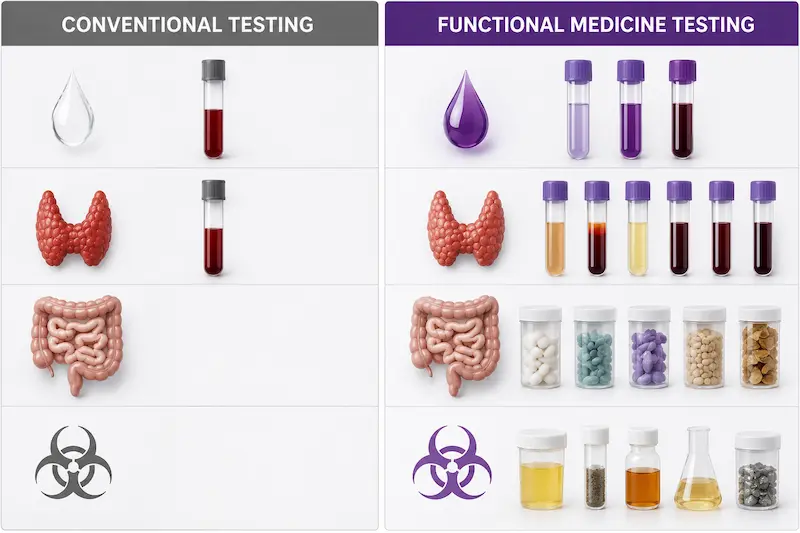
The Testing Gap: What Conventional Medicine Measures vs. What Functional Medicine Investigates
Panel by panel, here is what conventional testing typically runs, what it misses, and what functional medicine measures instead:
Blood Sugar and Metabolic Health
Conventional testing typically measures fasting glucose — a single-point measurement of blood sugar after an overnight fast. This is the most incomplete metabolic assessment available, for two reasons. First, the conventional fasting glucose reference range has broadened significantly over decades as the population average has shifted upward — meaning a result that would have been flagged as concerning twenty years ago now falls comfortably within “normal.” Functional medicine uses a tighter range that reflects optimal metabolic function rather than population average.
Second — and more clinically important for rosacea — fasting glucose can appear completely normal even when insulin resistance is actively developing. The pancreas compensates for early insulin resistance by producing more insulin to maintain glucose control, keeping glucose in the normal range while insulin levels are significantly elevated. Without fasting insulin measured simultaneously, this early-stage insulin resistance is entirely invisible to standard testing. HbA1c — which reflects average blood glucose over the previous three months and would capture the pattern that a single fasting glucose reading misses — is rarely ordered in conventional primary care, and yet metabolic dysregulation is one of the most consistent hallmarks of rosacea development, progression, and exacerbation I see in clinical practice.

Thyroid
Conventional thyroid assessment typically includes TSH only, sometimes with T4. This is inadequate for the rosacea clinical picture for multiple reasons. The conventional reference range for TSH flags hypothyroidism only at levels above 4.2-4.5 mU/L — a threshold established by population averaging rather than optimal function. Functional medicine flags suboptimal thyroid function at TSH above 2.0 mU/L, because this is where symptoms of thyroid insufficiency begin to appear and where thyroid-driven immune dysregulation, impaired gut motility, reduced DAO production, and slowed detoxification begin to affect rosacea.
Research published in Frontiers in Endocrinology highlights an additional critical concern: a significant number of patients — up to 30% — with TSH above 3.0 mU/L have occult autoimmune thyroid disease (Hashimoto’s thyroiditis) that is entirely invisible to TSH-only testing. Anti-TPO and anti-thyroglobulin antibodies must both be run simultaneously to capture this picture — and neither is included in a standard thyroid panel. A rosacea patient whose TSH is 3.2 — “normal” by conventional standards — may have active Hashimoto’s driving the immune dysregulation behind her skin inflammation, and would never know it from a standard panel.
Micronutrient Status
Conventional medicine rarely measures micronutrient status at all, and when it does, it measures serum levels — what is circulating in the blood — rather than cellular levels, which reflect what is actually available inside cells where nutrients do their biological work. A patient can have serum levels that appear adequate while cellular deficiency of B6, vitamin C, zinc, vitamin A, magnesium, or vitamin D impairs the specific enzymatic functions — DAO enzyme activity to degrade histamine, Treg synthesis, thyroid hormone conversion, collagen production — that are most relevant to rosacea. The Micronutrient Panel with SNPs measures cellular nutrient status alongside the genetic variants affecting how nutrients are absorbed, converted, and utilized — revealing the functional nutrient picture that serum testing consistently misses.
Gut Health
There is no standard conventional test for gut microbiome status, intestinal permeability, or dysbiosis unless symptoms are severe enough to warrant gastroenterology referral for a colonoscopy or endoscopy. The gut dysfunction driving the majority of rosacea cases I see — dysbiosis, H. Pylori infection, parasitic burden, SIBO, leaky gut — is entirely invisible to standard testing because standard testing does not look for it. The Gut Zoomer assesses 300+ microbiome markers, pathogen burden, digestive markers, and gut inflammation markers that would require no investigation at all under conventional protocol.
Toxic Burden
Heavy metals are tested in conventional medicine only in cases of acute poisoning. Mycotoxins from mold exposure and environmental chemical burden are essentially never assessed in conventional primary care or dermatology. And yet in my clinical practice, Total Tox Burden testing reveals significant heavy metal, mycotoxin, and environmental chemical burden in the overwhelming majority of rosacea patients I assess — toxic burden that is priming the immune system for the chronic hypervigilance that drives mast cell activation, histamine overload, and the inflammatory cascade visible on the skin.
Hormonal Picture
Standard hormonal assessment in conventional medicine typically consists of a single serum estrogen and progesterone measurement — a snapshot that captures circulating hormone levels at one point in time without assessing how estrogen is being metabolized or cleared. The Hormone Zoomer provides 24-hour urinary estrogen metabolites across the full estrogen pathway, progesterone, cortisol patterns across the day, melatonin, androgens, and DHEA — revealing whether estrogen dominance is driven by poor liver clearance, disrupted estrobolome function, xenoestrogenic chemical burden, or progesterone insufficiency. None of these distinctions are visible on a standard serum panel.
Why Did My Rosacea Suddenly Get So Much Worse? The Final Straw Concept
A question I hear consistently from patients whose rosacea has recently escalated significantly: “nothing changed — why is it suddenly so much worse?” The answer almost always involves the same clinical principle: something did change, and it was the final straw that broke the camel’s back.
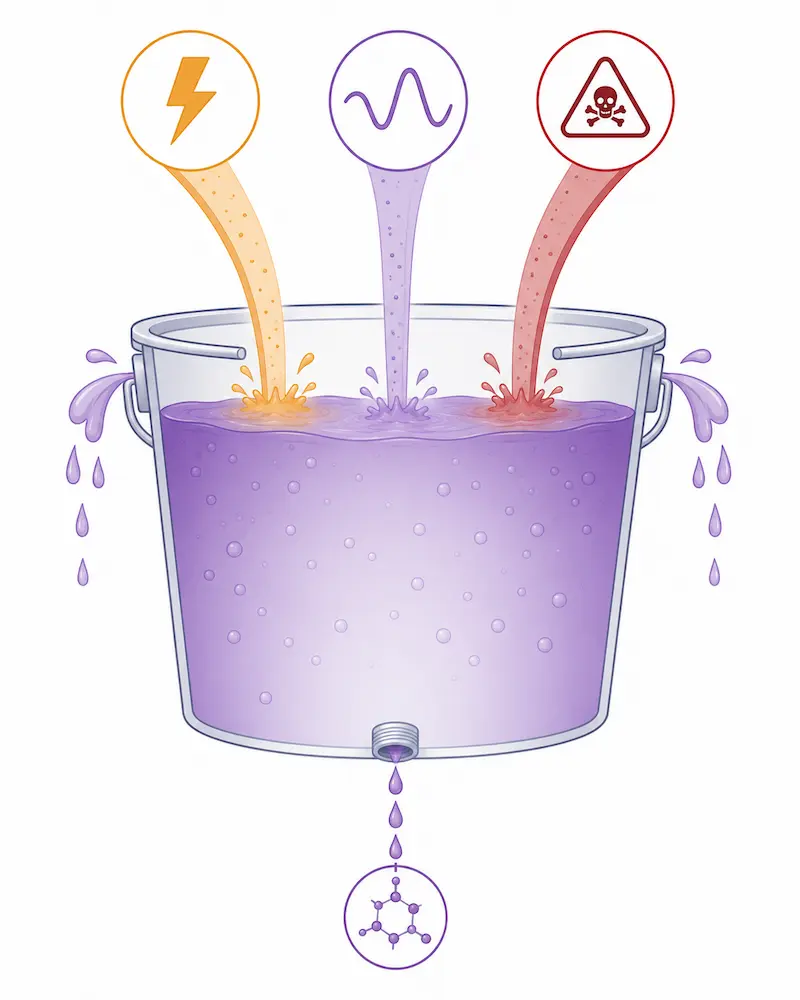
Rosacea does not worsen randomly. It worsens when the internal burden — the accumulated load of gut dysfunction, toxic exposure, hormonal imbalance, nutrient insufficiency, and immune dysregulation — exceeds the body’s current compensatory capacity. For years, the body may maintain a fragile equilibrium in which the rosacea is present but manageable. Then a new factor is added — not necessarily a large one — that pushes the bucket over the threshold. The new factor gets the blame because it coincided with the worsening. But the real story is the accumulated burden that was already at capacity before the final straw arrived.
The most consistent precipitating factors I see in clinical practice include:
Emotional and physiological stress — a major life stressor, a period of sustained work pressure, a significant loss, or an acute illness. Stress depletes vitamin B6, vitamin C, and other DAO cofactors while simultaneously elevating cortisol, raising TBG, reducing free thyroid hormone, and impairing the gut motility and barrier function that DAO production depends on. A patient whose rosacea was manageable can find it becoming significantly worse within weeks of a sustained stress period for these compounding biochemical reasons.
New gut dysbiosis — particularly parasitic infection acquired during travel, or candida overgrowth triggered by a combination of emotional stress, dietary changes, and antibiotic use. Parasitic infection impairs DAO production, increases histamine load, sequesters heavy metals, and amplifies systemic immune activation simultaneously — one of the most consistent “final straw” triggers I identify in patients whose rosacea escalated after an international trip or an illness requiring antibiotic treatment.
Perimenopause onset or poor estrogen clearance — the declining progesterone of perimenopause removes its mast cell-stabilizing effect while leaving estrogen’s mast cell-stimulating action unopposed. This can begin as early as the mid-30s and is one of the most consistent triggers for a patient whose rosacea was previously manageable suddenly becoming significantly worse. Poor estrogen clearance from impaired liver detoxification or a disrupted estrobolome produces the same estrogenic mast cell stimulation regardless of age.
Hormone replacement therapy without bioidentical progesterone — one of the most clinically significant and most consistently overlooked triggers I see. Conventional HRT using synthetic progestins or estrogen-only replacement without balanced bioidentical progesterone can significantly worsen rosacea by amplifying the estrogenic mast cell stimulation without providing progesterone’s regulatory counterbalance. This is precisely why urinary hormone testing through the Hormone Zoomer is imperative for any rosacea patient who has introduced HRT and noticed subsequent worsening — serum testing cannot reveal the metabolic picture that explains the trigger.
Toxic overload accumulation — toxic burden rarely produces a dramatic acute worsening event. More typically, it accumulates gradually until a threshold is crossed at which the immune system’s compensatory capacity is exceeded and the clinical picture shifts. A patient may have been managing mercury exposure from amalgam fillings or mycotoxin exposure from a water-damaged building for years before the accumulated burden crosses the threshold that pushes her rosacea from manageable to significantly worse. The trigger is the threshold, not the exposure itself.
Why the Longer This Goes Uninvestigated, the Harder It Becomes to Reverse
Worsening rosacea is not a random or inevitable progression. It is the immune system communicating upstream overwhelm — consistently, purposefully, and with increasing urgency. The longer the upstream picture goes uninvestigated, the more entrenched the internal environment becomes, and the more the threshold for reactivity lowers until the immune system is responding to stimuli it should be able to tolerate without effort.
Every year that the metabolic dysfunction, thyroid insufficiency, gut dysbiosis, and toxic burden underlying rosacea progression remain unaddressed, the internal environment becomes more self-reinforcing. Gut damage impairs the nutrient absorption needed to repair the gut. Nutrient insufficiency impairs the detoxification needed to clear the toxins worsening the nutrient insufficiency. Thyroid insufficiency slows the gut motility that allows dysbiosis to establish itself more deeply. The immune dysregulation that began as rosacea creates the conditions in which autoimmune progression becomes increasingly likely.
And critically — entering perimenopause with this picture already in place amplifies every driver simultaneously. The hormonal shift of perimenopause removes the mast cell-stabilizing effect of progesterone, worsens insulin sensitivity, reduces immune competence, and impairs detoxification — while the toxic burden that has been accumulating may simultaneously be accelerating the onset of perimenopause itself by disrupting hormonal signaling and ovarian function. The urgency of upstream investigation is not abstract. It is the clinical reality of what happens when the camel’s back is asked to carry increasing load without any of it being addressed.
Your worsening rosacea is not a skin problem that needs a better topical. It is a signal from an immune system that is asking for upstream investigation. The investigation is available. The findings are actionable. And the window for the most complete reversal is earlier rather than later.
→ Book your Initial Functional Medicine Health and Skin Assessment
P.S. If finances have been the only thing standing between you and starting your functional medicine journey — flexible payment options are available through Cherry. No interest, no impact on your credit score, quick approval, and affordable monthly payments. Apply in minutes on our website.
Frequently Asked Questions
Q1: Why is my rosacea getting worse even though my blood tests are normal?
Because “normal” on a standard blood panel means average — not optimal. Research shows that only 6.8-12.2% of American adults have optimal metabolic health, meaning the reference range for normal is built from a population in which nearly 93% have some level of metabolic dysfunction. Functional medicine uses tighter reference ranges built around optimal function, and investigates markers — fasting insulin, full thyroid panel with both antibodies, cellular micronutrient status, gut microbiome, toxic burden, and urinary hormone metabolites — that standard testing never runs. Worsening rosacea with normal conventional tests almost always reflects findings in these uninvestigated areas rather than the absence of findings.
Q2: What blood tests should I actually get for rosacea that my doctor hasn’t run?
A functional medicine rosacea workup goes significantly beyond standard panels. The most consistently informative testing includes: fasting glucose, fasting insulin, and HbA1c together (not fasting glucose alone); full thyroid panel including TSH, T4, T3, free T3, free T4, reverse T3, anti-TPO, and anti-thyroglobulin antibodies simultaneously; Micronutrient Panel with SNPs for cellular nutrient status and genetic variants affecting absorption; Gut Zoomer for microbiome assessment, H. Pylori, parasites; Wheat Zoomer for intestinal permeability; Total Tox Burden for heavy metals, mycotoxins, and environmental chemicals; and Hormone Zoomer for 24-hour urinary estrogen metabolites, progesterone, androgens, and cortisol. Every workup is individualized based on symptom picture and health history.
Q3: What causes sudden severe rosacea flare-ups after years of relative stability?
Sudden significant worsening almost always reflects the ‘final straw’ principle — the internal burden was already at capacity, and a new factor pushed the bucket over the threshold. The most consistent precipitating factors include sustained emotional or physiological stress (depleting DAO cofactors and impairing thyroid and gut function simultaneously), new gut dysbiosis from travel-acquired parasites or candida overgrowth, perimenopause onset removing progesterone’s mast cell-stabilizing effect, introduction of HRT without bioidentical progesterone amplifying estrogenic mast cell stimulation, and toxic burden accumulation crossing the immune system’s compensatory threshold. The new factor gets the blame because it coincided with the worsening, but the accumulated internal burden that was already at capacity is the real story.
Q4: Can insulin resistance make rosacea worse even when fasting glucose looks normal?
Yes — and this is one of the most consistently missed metabolic findings in rosacea patients. The pancreas compensates for early insulin resistance by producing more insulin to maintain glucose control, keeping glucose in the normal range while insulin levels are significantly elevated. Without fasting insulin measured simultaneously alongside fasting glucose and HbA1c, early-stage insulin resistance is entirely invisible to standard testing. Metabolic dysfunction — including subclinical insulin resistance — is one of the most consistent hallmarks of rosacea development and exacerbation, which is why the functional medicine metabolic assessment runs all three markers together rather than relying on fasting glucose alone.
Q5: Can HRT make rosacea worse?
Yes — particularly when HRT is introduced without bioidentical progesterone in combination with poor estrogen clearance. Conventional HRT using synthetic progestins or estrogen-only replacement without balanced bioidentical progesterone can significantly worsen rosacea by amplifying estrogenic mast cell stimulation without providing progesterone’s mast cell-stabilizing counterbalance. This is one of the most consistently overlooked triggers for rosacea worsening in perimenopausal patients. Urinary hormone testing through the Hormone Zoomer is essential for any rosacea patient who has introduced HRT and noticed subsequent worsening — serum hormone testing cannot reveal the metabolic and clearance picture needed to explain and address the trigger.
Q6: Does rosacea get worse without root cause investigation?
In my clinical experience, yes — consistently. The internal drivers of rosacea — gut dysbiosis, metabolic dysfunction, thyroid insufficiency, toxic burden, nutrient depletion, and hormonal imbalance — do not resolve on their own and tend to become more entrenched over time as each driver compounds the others. The gut damage that impairs nutrient absorption worsens the nutrient insufficiency that impairs gut repair. The thyroid insufficiency that slows detoxification worsens the toxic burden that impairs thyroid function. Without upstream investigation and targeted intervention, the internal environment that drives rosacea continues to develop — and the threshold for immune reactivity lowers progressively until the condition becomes significantly harder to reverse than it would have been at an earlier stage of investigation.
Written by Natalie Maibenko – a Certified Functional Medicine Practitioner and Master Esthetician with 22+ years of experience and founder of Unique Verve

As a Certified Functional Medicine Practitioner my Expertise Encompasses:
- Immune System: frequent illness, UTIs, yeast infections
- Allergies, Asthma
- Skin Problems: acne, cystic acne, rosacea, eczema, dermatitis, ichthyosis, psoriasis, vitiligo, melasma
- Inflammation: arthritis, rhinitis, joint & muscle pain, migraines, headaches
- Sleep Disturbunces, Insomnia
- Gut Problems: IBS/IBD, bloating, acid reflux, gas, constipation, diarrhea, parasites, fungal/yeast overgrowths
- Hormonal Imbalances: PCOS, PMS symptoms, weight problems/inability to lose weight, thyroid problems
- Hair Loss, Alopecia
- Mood Imbalances: anxiety, depression, irritability
- Metabolic Dysfunction, Insulin Resistance, Type 2 Diabetes
- Optimizing Wellness for Successful Pregnancy
- Autoimmune Conditions: Hashimoto’s thyroiditis, grave’s disease, reumatoid arthritis (RA), lupus, etc
- Bone Health: osteopenia/ osteoporosis
- Effective Anti-Aging Strategies without Injectables with the inside-out & outside-in approach
- Detoxification of Heavy Metals, Mycotoxins, Environmental Toxins
- Reversing Breast Implant Illness
- Preparation for the Explant Surgery and Optimization of Wellness & Vitality Post-Explant
With love and gratitude,
Natalie Maibenko
Functional Medicine & Skincare Expert – Helping You Take Control of Your Health and Achieve Lasting Skin Results Nationwide — Virtual Practice